
Download as PDF, PPTX
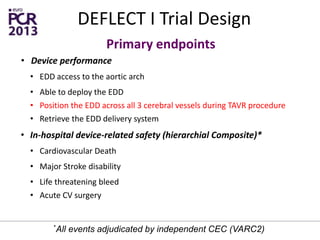
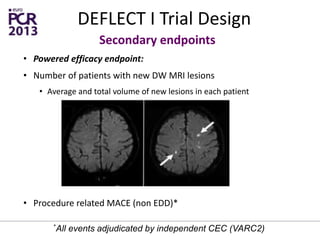

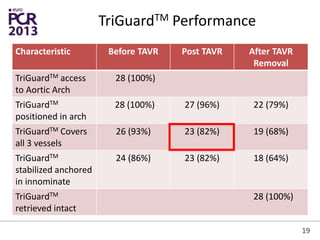
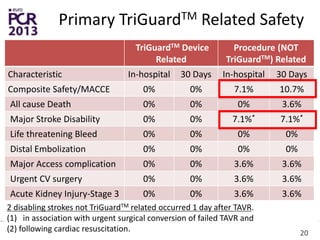
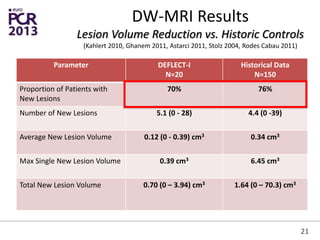
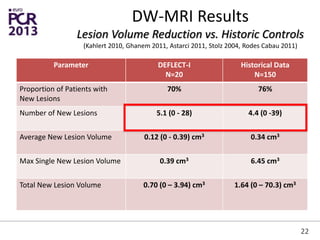
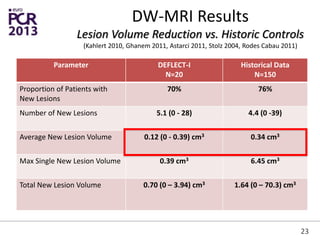
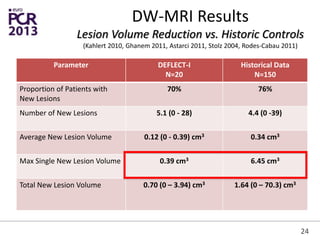
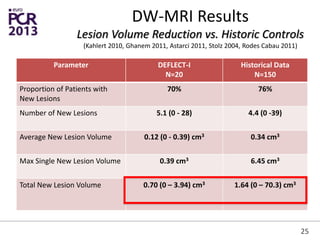
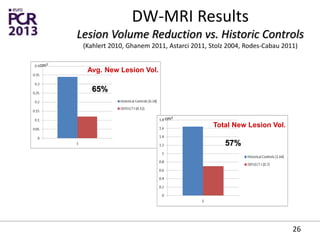
The DEFLECT I trial evaluated the safety and performance of the TriGuard embolic deflection device in patients undergoing TAVR. The study found: 1) The TriGuard device was successfully deployed and retrieved in most cases without any device-related complications. 2) Rates of new brain lesions following TAVR with TriGuard were similar to historical controls, but the average and total volumes of new lesions were significantly lower (reduced by 65% and 57% respectively) compared to historical data. 3) The results provide preliminary evidence that the TriGuard device may help reduce the volume of cerebral embolic material and ischemic brain injuries during TAVR without increasing safety risks. Larger studies are still needed























































































