

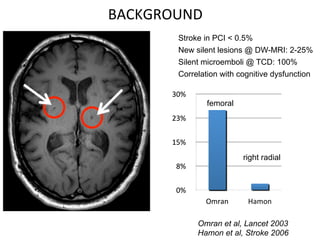
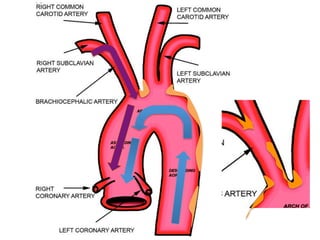
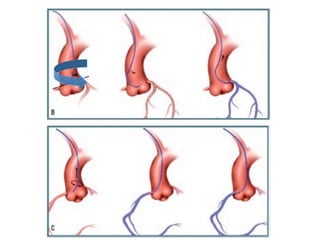
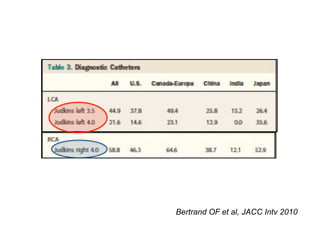
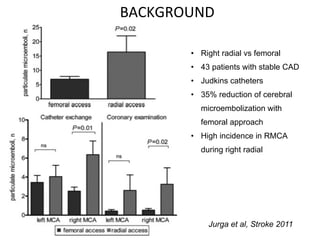
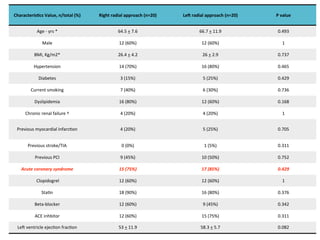
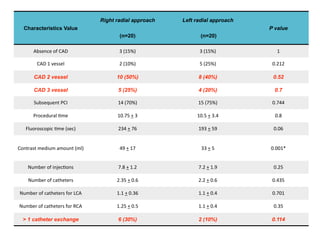
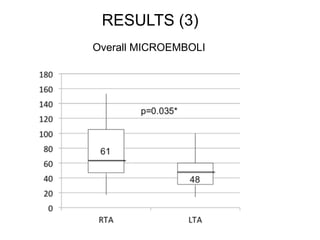
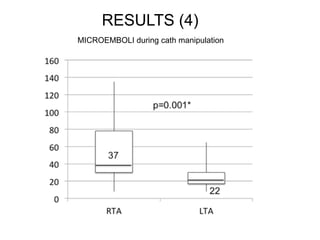
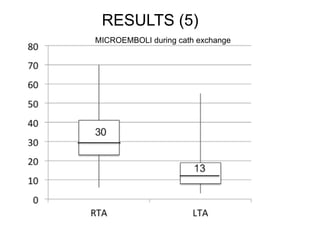
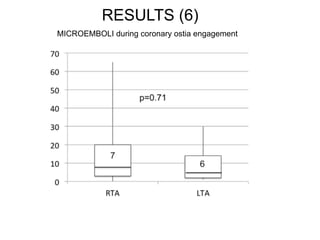
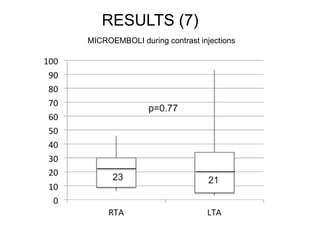
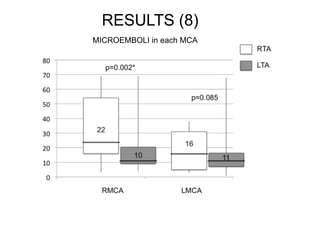
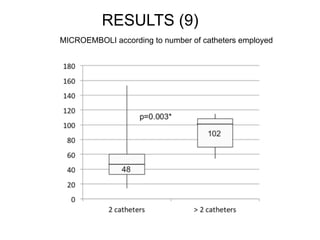
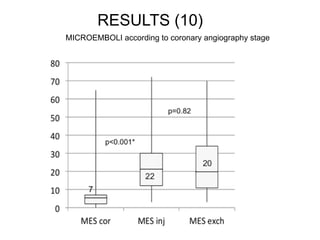

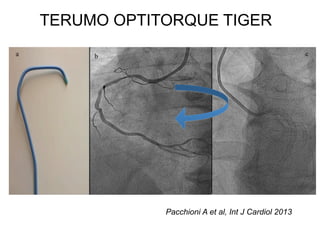
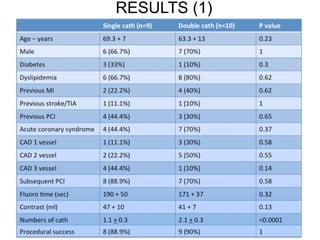
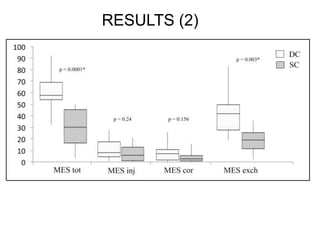
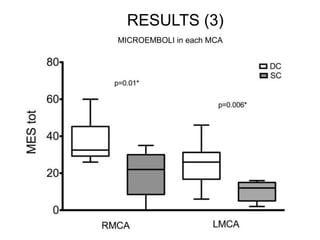
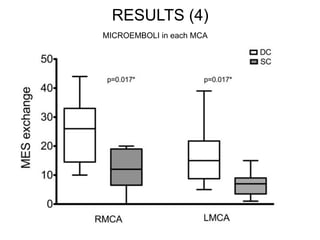
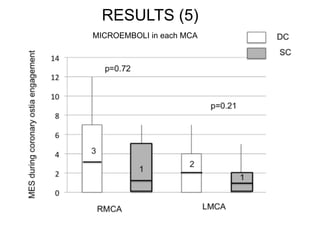

This document compares the risk of microembolization during diagnostic coronary angiography between single catheter and double catheter strategies. In the first study, a left radial approach was found to have a lower rate of microembolization than a right radial approach, likely due to less catheter manipulation and exchanges. Independent predictors of high microembolization included a greater number of catheters used. A second study found that using a single "Tiger" catheter halved the rate of microembolization compared to using a double catheter "Judkins" strategy, mainly by reducing catheter exchanges. Minimizing catheter exchanges may help reduce the risk of air embolism and microembolization during coronary angiography procedures.











































































































