Downloaded 399 times








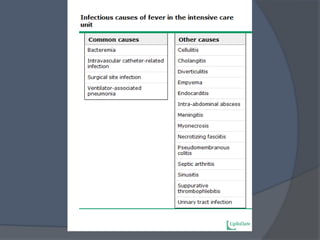









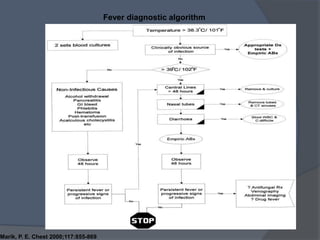



The hypothalamus controls body temperature through neurons that receive signals from temperature receptors in the skin and blood. These signals are integrated in the hypothalamus' temperature regulation center to maintain a normal temperature of around 37°C. Fever is defined as a temperature greater than 37.2°C in the morning or 37.7°C in the afternoon. Common causes of fever in the ICU include infections like ventilator-associated pneumonia as well as non-infectious causes like drug reactions. Blood cultures, sputum cultures, urine cultures and imaging tests may help diagnose the cause, and treatment is aimed at the underlying condition.