Downloaded 65 times





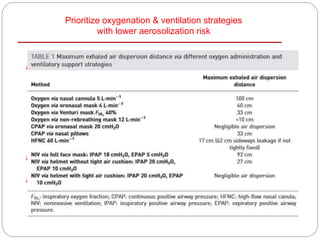
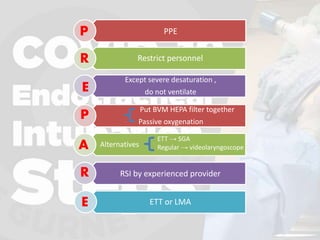
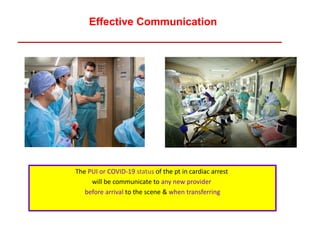

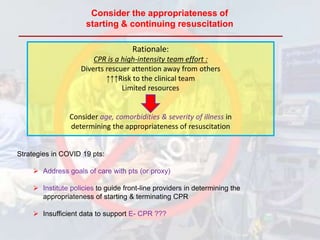
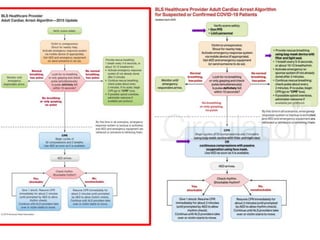
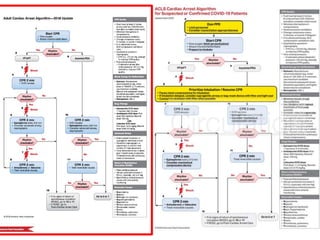


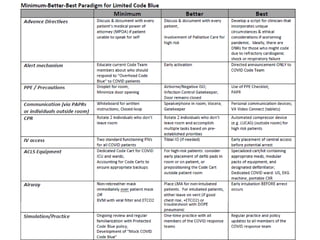
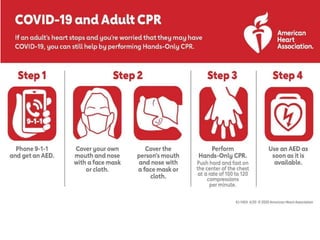
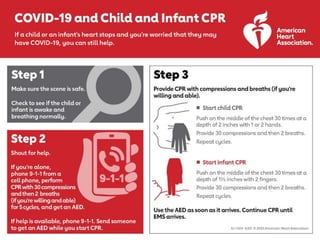
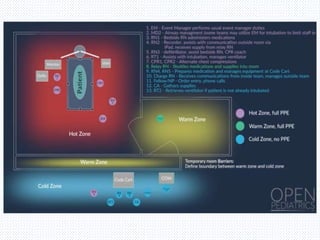
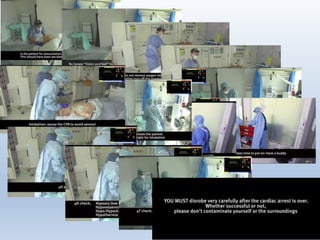
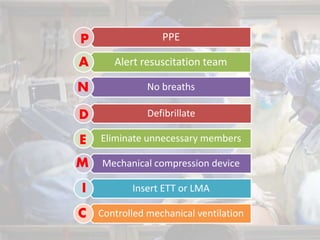

The document discusses CPR protocols during the COVID-19 pandemic, emphasizing the increased risks to healthcare workers due to aerosol-generating procedures. It outlines guidance from various resuscitation organizations on adapting CPR practices in both in-hospital and out-of-hospital settings, including the use of personal protective equipment (PPE) and considerations for patient assessment. Key recommendations include limiting personnel involved in resuscitation efforts, prioritizing communication about COVID-19 status, and modifying ventilation strategies to minimize aerosol exposure.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














