Downloaded 34 times



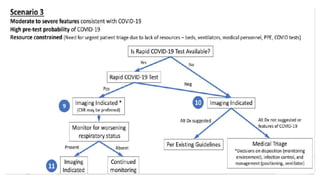

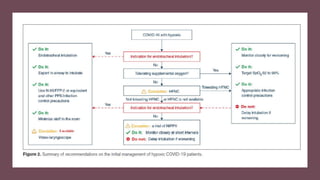
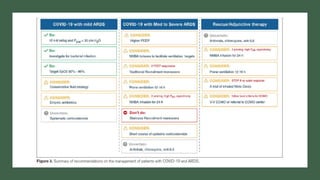



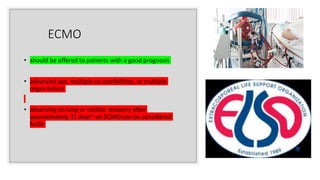
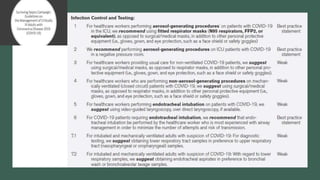


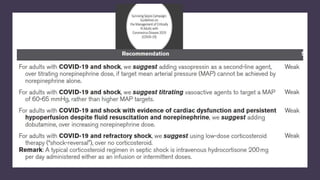



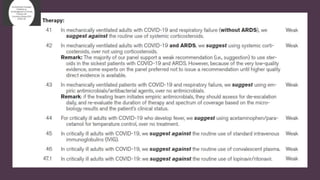
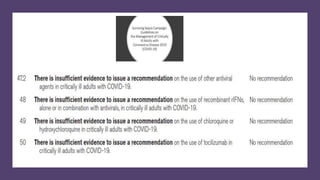
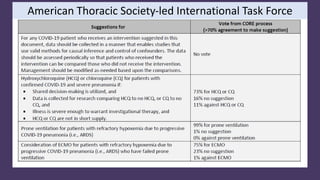
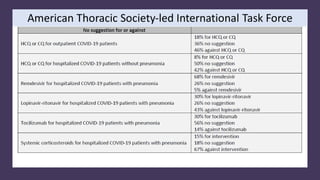
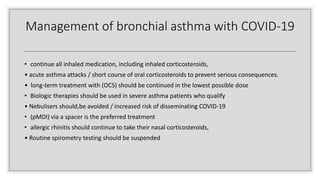
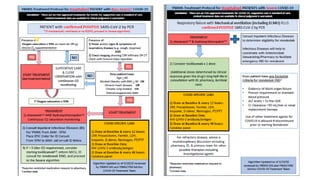
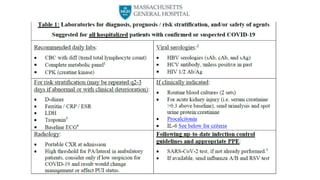
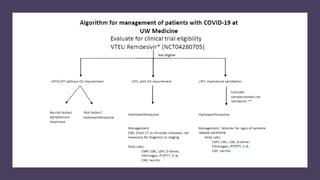


The document summarizes information and recommendations regarding the Covid-19 pandemic from the perspective of intensive care and critical care specialists. It provides worldwide case statistics and projections for hospital bed and ventilator needs in California. Guidelines are presented on testing, diagnosis, treatment strategies including ventilation, use of sedatives, ECMO, and experimental drugs. Risk stratification, PPE guidance, and management of complications like shock are also addressed. Clinical trials and the potential use of convalescent plasma are discussed.











































































