



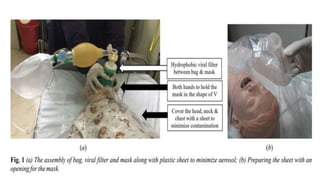
![Intubation
• During the previous SARS epidemics in China and Singapore, infection
rates were higher in doctors and nurses carrying out endotracheal
intubation [relative risk (95% CI)-13.3 (2.99–54.04)].
• In an observational study of influenza-A and influenza-B in exhaled
breath, viral RNA was seen in one-third of infected patients and 99%
of particles had a diameter of approximately 125 nm (0.125 µm).](https://image.slidesharecdn.com/covid19-paeds-200610171153/85/Managing-pediatric-Covid-19-client-on-ventilator-26-320.jpg)


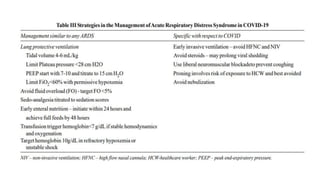


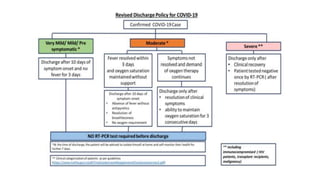




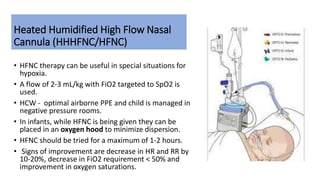
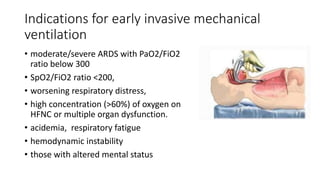
- Pediatric COVID-19 patients may require intensive care management including ventilator support for ARDS and multi-organ dysfunction. The document outlines guidelines for managing pediatric COVID-19 patients who require ventilation, including use of low-flow oxygen devices, criteria for intubation and mechanical ventilation, and strategies to prevent complications like ventilator-associated pneumonia. Key aspects of care include supportive therapy, infection control, and addressing challenges of limited resources and healthcare worker stress and burnout.























































































