Anatomy of crystalline lens by Dr. Aayush Tandon
•
51 likes•13,173 views

The document summarizes the anatomy of the crystalline lens. It discusses the lens's structure, composition, dimensions, and surgical anatomy. Key points include: - The lens is a transparent biconvex structure composed mainly of specialized cells and proteins. It helps focus light onto the retina to allow vision. - Structurally, it has an outer lens capsule enclosing lens epithelium cells and elongated lens fibers in concentric layers. The fibers are arranged in a nucleus and surrounding cortex. - Dimensions vary with age but the lens is roughly 10mm in diameter and weighs around 258mg in adults. It provides around 16-17 diopters of refractive power and accommodates vision changes. - Surgically

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Anatomy of crystalline lens by Dr. Aayush Tandon
Similar to Anatomy of crystalline lens by Dr. Aayush Tandon (20)
Recently uploaded
Recently uploaded (20)
Anatomy of crystalline lens by Dr. Aayush Tandon
- 1. Dr. Aayush Tandon Anatomy of the Crystalline lens
- 2. It is a highly organised system of specialsed cells. It constitutes an important component of the optical system of the eye. Introduction 1. It allows the passage of incident light to the retina as it is transparent. 2. It enables the eye to focus the images of the objects on the retina lying at distances from near to infinity ( accomodation) 3. Lens helps in refraction of light and it constitutes one fourth of total diopteric power of the eye.
- 3. Anatomy It is a transparent, avascular, biconvex,semisolid,intraocular, crystalline structure placed between the iris and vitreous in a saucer shaped depression the patellar fossa. It is attached posteriorly to the vitreous in a circular manner with Ligamentum Hyaloideocapsulare also called Wiegerts`s ligament. Between the hyaloid face and lens capsule there there is a small potential space called retrolental or Bergers space. It is supported in its position by zonules of zinn or suspensory ligaments.
- 5. Like any other lens the crystalline lens has 2 surfaces , anterior and posterior Anterior surface is less convex as compared to the posterior surface The centre of anterior and posterior surfaces is called as the anterior and posterior pole respectively. The anterior pole is about 3mm from the back of cornea
- 6. The lens is unique among organs in that is contains cells solely of a single type , in various stages of cytodifferentiation and retains within it all the cells formed during life time . As cells become older and more embedded they undergo several changes, losing organelles and to some extent their structural integrity and becoming progressively more inert metabolically. As no cells are shed the lens demonstrates cells at varying states of senescence.
- 7. Dimensions 1. Radius of anterior surface - 10 mm (8-14mm) 2. Radius of posterior surface - 6 mm (4.5- 7.5mm) 3. Anterior pole- 3 mm from the back of cornea. 4. Equatorial diameter 6.5mm at birth 10mm in adults
- 8. 6. Axial width ( AP width) At birth- 3.5-4 mm In adults- 4.75- 5 mm 7.Refractive index of lens As a whole – 1.39 Nucleus – 1.42 Cortex- 1.38 8. Refractive power – 16-17 D 9. Weight of lens at birth- 65 mg at around 10 years 135 mg at extremes of age- 258 mg
- 9. 10. Accomodative power at birth - 14-16 D at 25 yrs - 7-8 D at 50 yrs - 1-2 D 11. Colour of lens Infants – Transparent Young adults - Colourless After about 30 yrs of age - yellowish tinge Old age- amber colour 12. Consistency of lens- Semisolid cortex is softer as compared to the nucleus
- 10. It is composed of 64% water,35% proteins and 1 % lipids, carbohydrates and other trace elements. Structure of lens: 1. Lens capsule 2. Lens epithelium 3. Lens Fibres
- 11. Lens capsule It is a thin , transparent, hyaline collagenous membrane which surrounds the lens completely. It is secreted by the basal cells of anterior lens epithelium anteriorly and by the basal area of elongating lens fibers posteriorly. It is the thickest basement membrane of body. It is an inverted basement membrane facing inside of closed cavity. It is more thick anteriorly than posteriorly and at equator than poles. It is thinnest at the posterior pole. It is mainly made up of of type-IV collagen and Glycomaminoglycans.
- 13. Capsule thickness increases anteriorly with age but there is little change at the posterior pole. On microscopy the capsule appears as a homogenous, transparent structure showing a Lamellar appearance with fibres arranged parallel to its surface
- 14. There are upto 40 lamellae , each of which is about 40 nm thick . The lamellar structure becomes modified with age since it disappears from the posterior pole during the first decade and from the anterior aspect four to five decades later. Basement membrane origins of the capsule are displayed by a positive PAS reagent which stains the glycoprotein matrix The capsule is permeable to water, ions and other small molecules and offers a barrier to large protein molecules.
- 15. Anterior lens epithelium It is a single layer of cuboidal nucleated epithelial cells. Contains all the organelles found in a typical epithelial cell Cells have a high metabolic rate ( content of ATP and enzymes highest in this area of lens Almost all metabolic, synthetic and transport process of lens occurs here. In the equatorial region these cells become columnar and are actively dividing and elongating to form new lens fibres through out life There is no corresponding posterior epithelium
- 16. There are about 500000 epithelial cells in a mature lens . These cells have a prominent well characterised cytoskeleton network consisting of Actin , myosin. Alpha actinin , vimentin , spectrin & microtubules . This well defined cytoskeleton compartmentalizes the cell interior . The cytoskeletal network is in the form of polygonal array of geodomes located subjacent and attached to their apical membrane .
- 18. Central zone :- It consists of cuboidal cells. These cells are stable and their number reduces with the age. Normally, these cells do not mitose. But can do so in response to various insults like uveitis, atopic dermatitis. Intermidiate zone :- It contains small but more cylindrical cells. They can mitose occasionally. Germinative zone :- It consists of coloumnar cells. These are actively dividing and elongating to form new lens fibres. Very susceptible to irradiation.
- 20. PSC
- 21. Lens fibres Anterior lens epithelium elongates to form the lens fibres. They form the main bulk of the lens They are long thin transparent cells firmly packed with diameter of 4-7 micron and length upto 12mm New cell fibres are laid on the older deeper fibres Superficial new fibres are nucleated with elongation of the cell The nuclei assume a more anterior position Anterior shifted nucleus of the newly formed cells form the line convex forward at equator, called as nuclear or lens bow.
- 23. On cross section the lens fibres are hexagonal in shape and are bound together by ground substance . The cytoplasm of lens fibres are devoid of nuclei with very few organelles
- 24. There are interlocking processes between cells as ball-and-socket and tongue-and-groove interdigitations. Interdigitations are less complicated in superficial zone to permit moulding of the lens in accomodation. Lens fibers exhibit numerous gap junctions
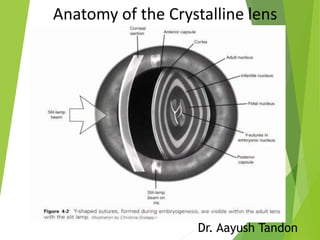
- 25. Initial fibres forming the foetal nucleus terminate with two Y-shaped sutures, anteriorly upright Y and posteriorly inverted Y.
- 26. In adults continuously forming fibres are arranged compactly as nucleus and cortex. With further growh there is symmetrical branching of sutures forming the 9 point star of the mature cortex
- 27. Nucleus : Central part containing the oldest fibres Parts of nucleus- 1. Embryonic nucleus (1-3 months of Gestation) 1. Fetal nucleus (3 months – birth) 2. Infantile nucleus (Birth- puberty) 3. Adult nucleus.
- 28. Cortex Peripheral part It has the youngest fibres. Histologically ,section through the equator shows the hexagonal structure of lens fibres and bound together by ground substance.
- 29. Surgical Anatomy
- 30. Grading of nucleus hardness Grade 1 – Green yellow Grade 2 – Yellow Grade 3 – Amber Grade 4 –Brown Grade 5 – Black
- 31. Ciliary Zonules The ciliary zonules ( Zonules of Zinn or Suspensory ligaments ) consist of a series of stiff, non elasitic fibres which run from ciliary body and fuse into the outer later of the lens capsule The ciliary epithelial cells of the eye probably synthesize portions of the zonules The zonules are primarily made of fibrillin, a connective tissue protein Each zonular fibre has a diameter of about 0.35 – 1 microns It is composed of microfibrils, glycoproteins and mucopolysaccharides They hold the lens in postion and enable the ciliary muscles to act on it
- 32. Gross appearance Grossly, the ciliary zonules from a complete ring of fibres, which extend from ciliary body to the lens equator circumferentially. On cut section the ciliary zonules appear to be arranged in a triangular form.
- 33. The base of the triangle is towards the equator of the lens and apex towards the ciliary body . As the zonular fibres insert on the lens capsule a narrow space is created around the equator which is called the ‘The canal of Hanover
- 35. Structurally , 3 different types of fibres- 1) First type fibres- thick,wavy and lie near vitreous. 2) second type fibres-thin and flat. 3) third type fibres- very fine & run circular course.
- 36. Arrangement of zonular fibres
- 38. THANK YOU
- 39. Arrangement of zonular fibres (New concept) > Majority of zonules arise from the posterior end of the pars plana upto 1.5 mm from the ora serrata > They run a continues course from ora serrata to the edge of lens
- 40. Applied Anatomy 1. Capsule 2. Superficial cortex : a) C1α- subcapsular clear zone b) C1β- first zone of disjunction seen as bright, narrow, scattering zone of discontinuity c) C2 – second cortical clear zone. 3. Deep cortex : a) C3 – bright light scattering zone b) C4- clear zone of cortex. 4. Nucleus.
- 41. In a can opener capsulotomy, improper joining of the radial cuts can lead to a pull on the still attached capsule, as it is removed causing a posterior extension of the tear Extension of the tear to the periphery may occur if the attempted rhexis size is larger than 6mm. If the CCC created is larger than the proposed optic size ,the odds of posterior capsular opacification are higher Creation of small rhexis (less than 4mm) carries a risk of fluid entrapment while performing hydrodissection leading to ruptureof the posterior capsule . Nucleus rotation in case of inadequate hydroprocedures can lead to zonular dialysis
Editor's Notes
- This causes any new lens fibres to be added on the inside of the lens
- This shows that the seceretory source of the basement membrane ( Anterior Epithelium) is itself situated anteriorly and is involved in remodelling of the lens capsule which occurs with lens growth .
- Albumin Mr 70kDA HB Mr 66,7 kDA
- There is no posterior epithelium as the cells are used up in filling the central cavity of the lens vesicle
- Central density of about 5009/mm2 in men and 5781/mm2 in women .
- Central Zone – Metplasia of these central zone epithelial cells can lead to Anterior subcapsular cataract eg. Shield cataract in Atopic dermatitis & glaukomflekon after acute attack of Acute angle closure glaucoma
- Dysplasia of these cells of the germinative zone can lead to PSC as seen in radiation cataract, myotonic dystrophy and neurofibromatosis type 2
- At first the lens fibres are forms from posterior epithelium but later on lens fibres are drived from the cells of the equatorial region of anterior epithelium
- Size of embryonic and fetal nucleus remain constant whie adult nucleus is always increasing This stratification is due to the optical difference between the older more sclerotic regions of central lens and newer transparent peripheral areas
- Important for setting the parameters of the machine for effective phacoemulsification
- Equatorial fibres are present in large numbers in young eyes but tend to become less numerous as age advances
- Orbiculo-posterior capsular fibres - most posterior and innermost fibres - origin- ora serrata - insertion- on posterior capsule of lens alonwith Weigerts ligament. - second type fibres Orbiculo-anterior capsular fibres -thickest and strongest - arise from pars plana - inserts anterior to the equator of lens - first type fibres Cilio-posterior capsular fibres- -most numerous zonular fibres - arise mainly from the valleys - inserts on posterior capsule Cilio-equatorial capsular fibres- -- arise from valleys of ciliary process - directly inserts on the equator of lens - third type of fibres - abundent in youthful eyes andreduces in number with advancing age
- Pars orbicularis – Arise from post end of pars plana ,pass forward over the plans plana Zonular Plexus – Reaching the post margin of of pars plicata the zonular fibres segment into zonular plexus which pass throught valleys between the ciliary process . Known as tension fibres Zonular fork – After reaching anterior margin of pars plicata fibres consolidate into budles which bend at right angle Zonular limbs Ant – analogous to orbicularis anterior fibres Equatorial – analogous to cilio equatorial fibres Posterior – Analogous to orbiculo posterior fibres
- Zonular dialysis likely to happen in presence tof capsule cortical adhesions