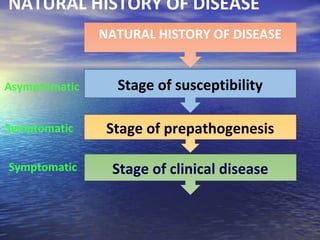
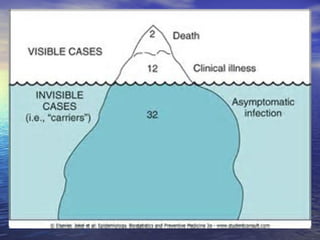
This document discusses several concepts related to disease causation and pathogenesis. It introduces theories of disease causation including the germ theory, biomedical model, and theories of multifactorial causation. It describes the epidemiological triad of agent, host, and environment. It also discusses the natural history of disease, including prepathogenesis and pathogenesis phases, and the iceberg phenomenon where most disease is hidden and subclinical.