Downloaded 181 times

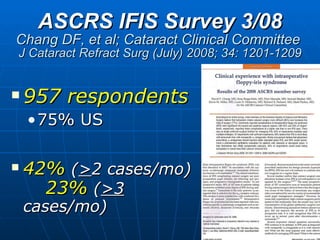
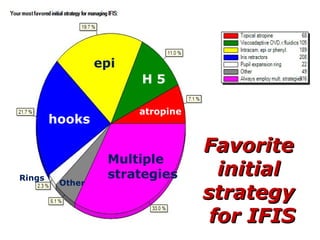
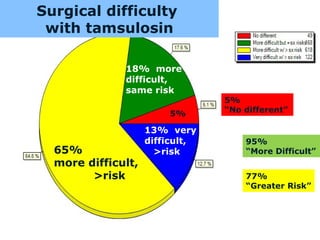
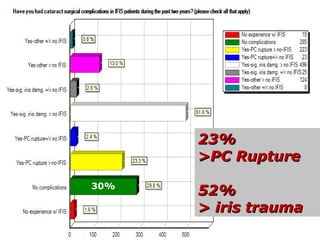
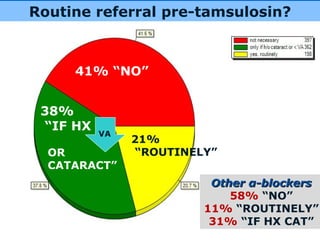
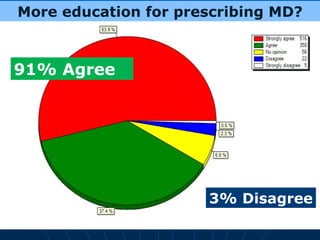
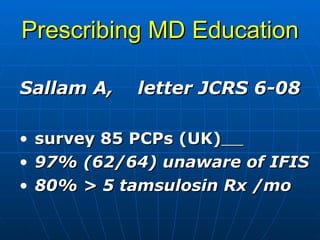
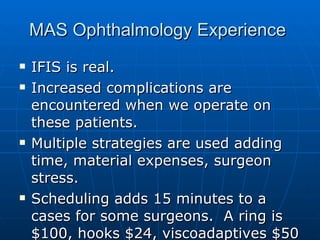

The document discusses Intraoperative Floppy-Iris Syndrome (IFIS), a condition characterized by a floppy iris that is more prone to prolapse during cataract surgery. IFIS is associated with the use of alpha-1 blockers like tamsulosin that are commonly used to treat benign prostatic hyperplasia. Surgery on patients with IFIS can lead to complications like iris trauma, dropped lens, and vitreous loss. Multiple strategies are used during surgery to manage a floppy iris, including pharmacologic agents, viscoelastic devices, and mechanical dilating devices. While IFIS increases surgical difficulty and risk, ophthalmologists and urologists can work together through education and alternative


















































![Ocular pharmacology [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/ocularpharmacologyautosaved-191124050400-thumbnail.jpg?width=640&height=640&fit=bounds)






















