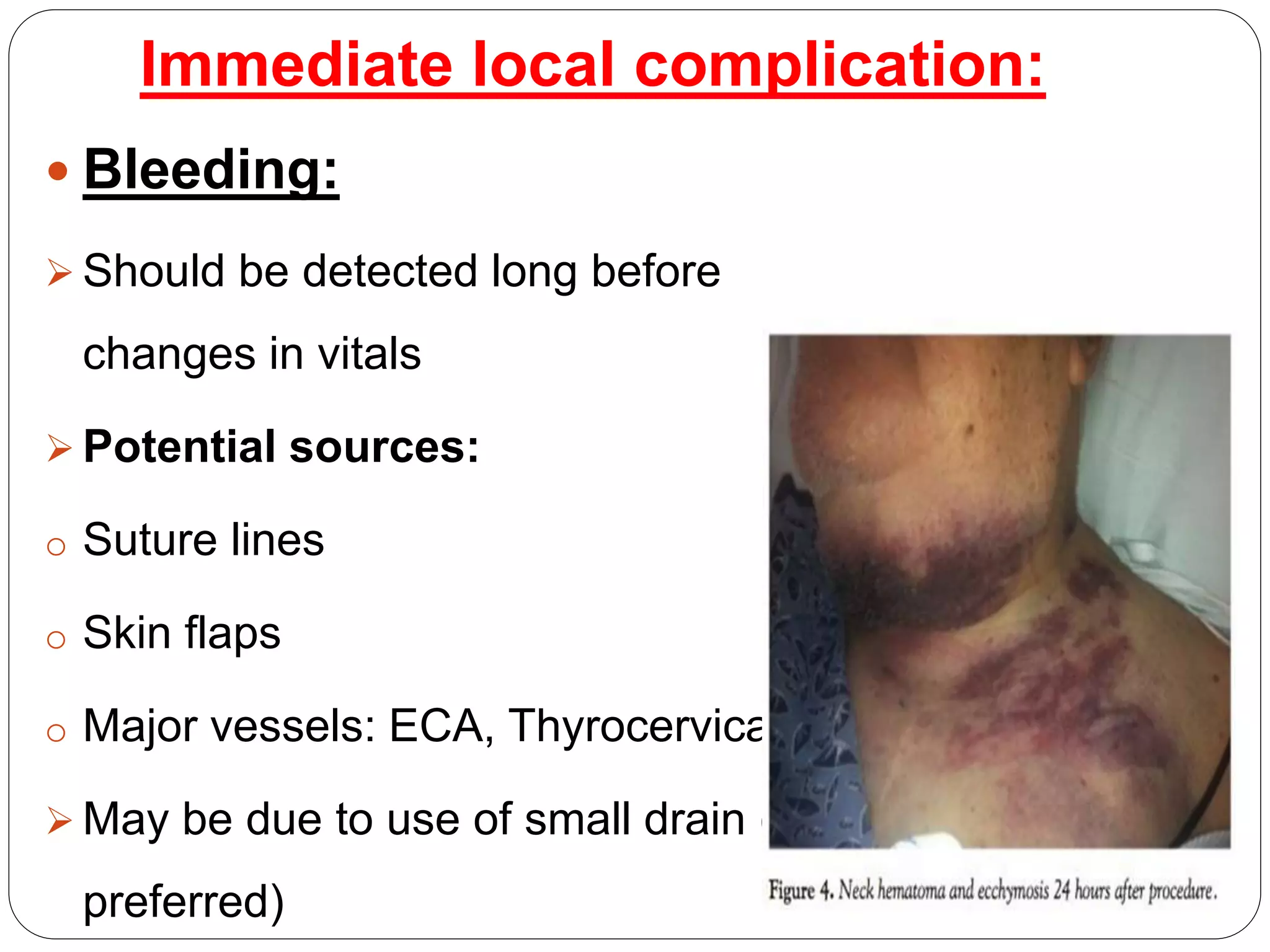
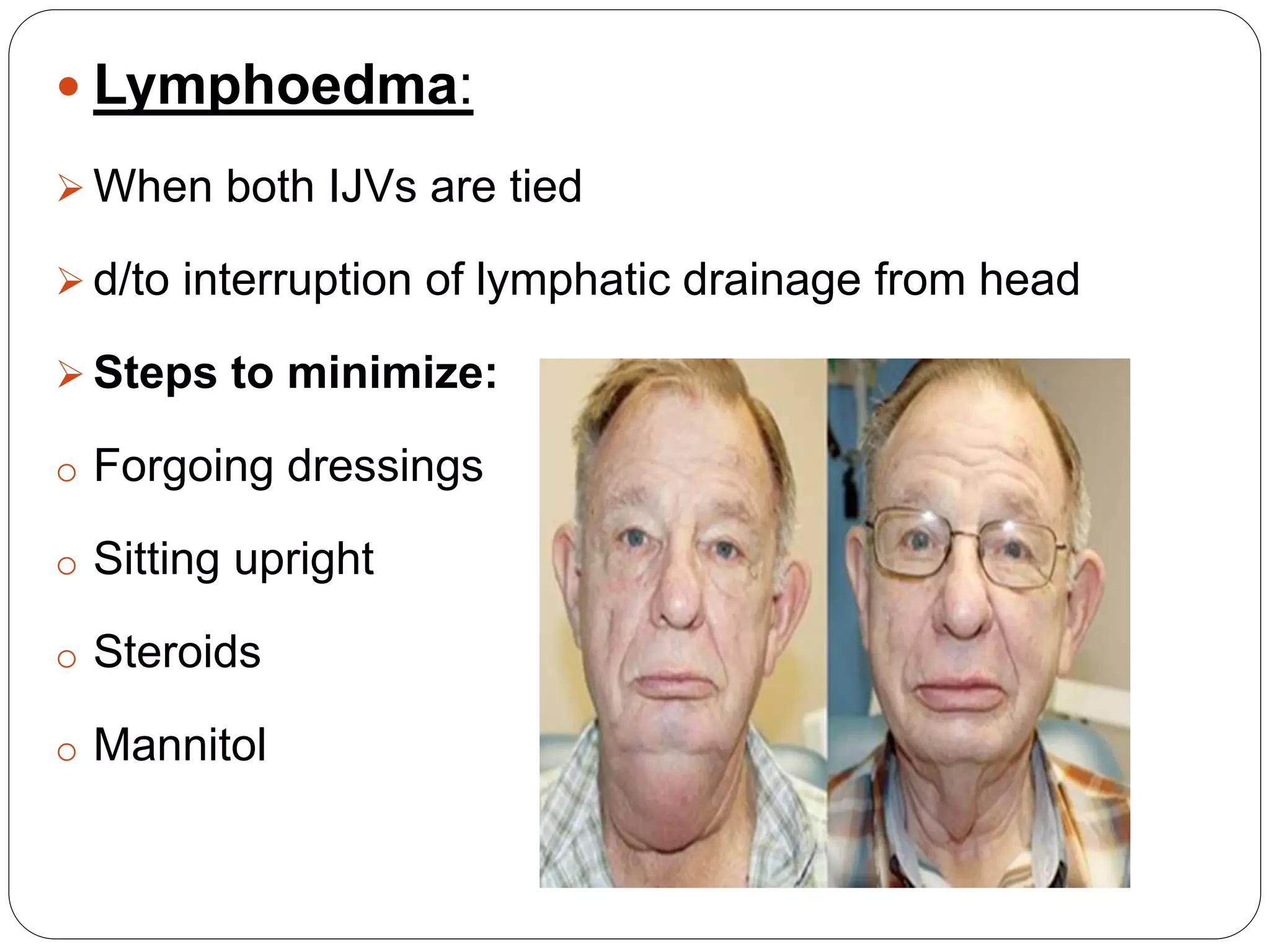
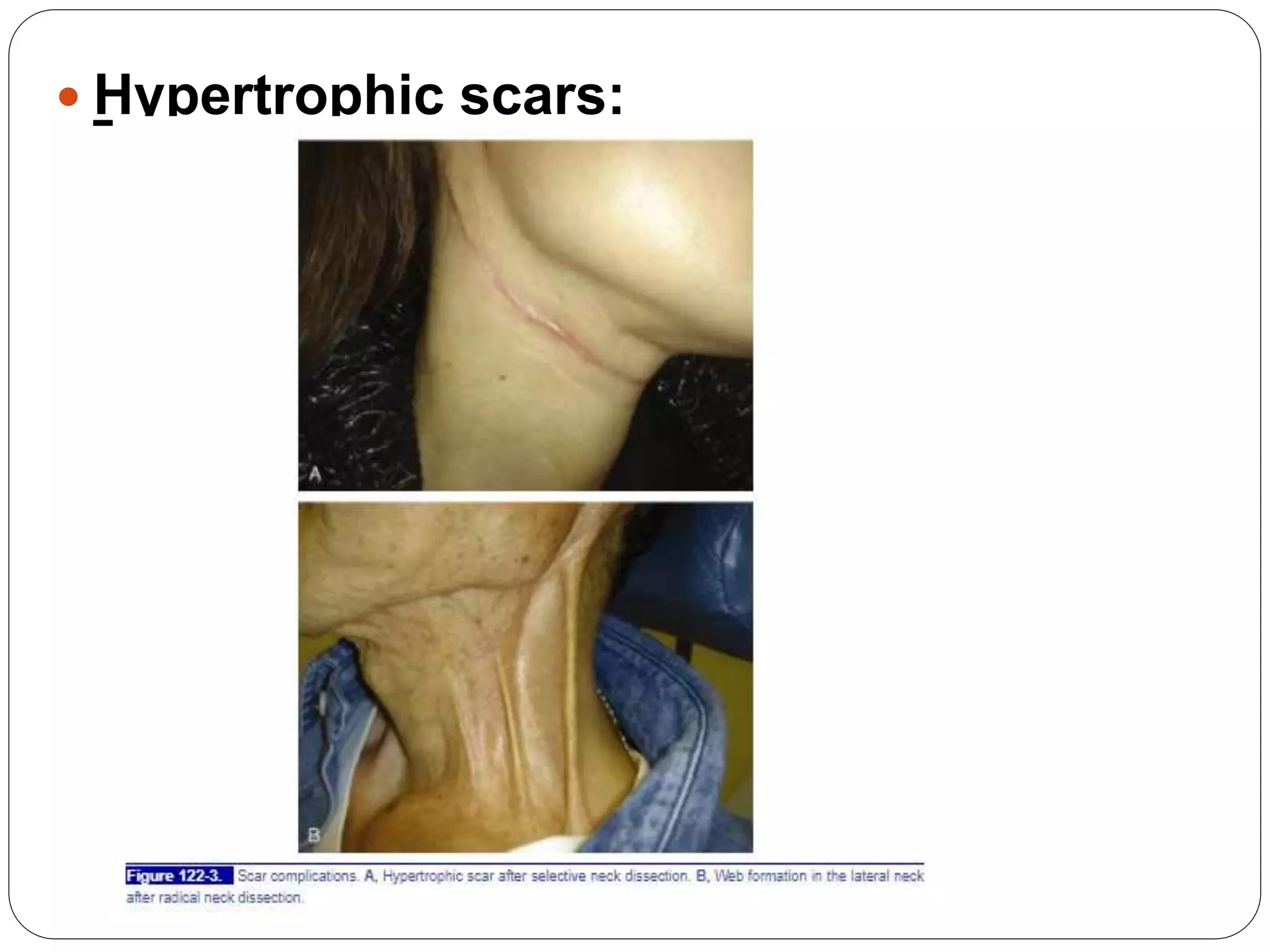
Dr. Sanjay Maharjan discusses complications that can occur following head and neck surgery like neck dissection. He classifies complications as major or minor, early or late, local or systemic. Some immediate local complications discussed include bleeding, shock, airway obstruction, and increased intracranial pressure. Intermediate complications include chylous fistula, seroma, wound infection, and flap failure. Late complications can include recurrence, parotid gland hypertrophy, lymphedema, and hypertrophic scarring. The document provides details on prevention, diagnosis, and management of various complications.