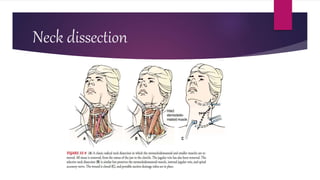
This document discusses neck dissection procedures. It begins with an introduction describing how cancer can metastasize to cervical lymph nodes. It then describes different types of neck dissections like radical and selective dissections. Complications from dissections like hemorrhage, nerve injury, and chyle fistulas are discussed. Reconstructive techniques using flaps and grafts are described. Nursing diagnoses and post-operative rehabilitation exercises are also summarized.