Downloaded 124 times
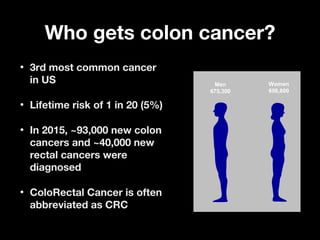
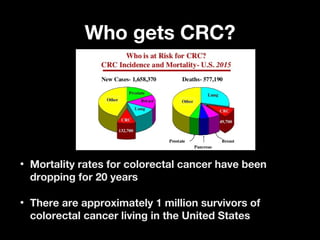
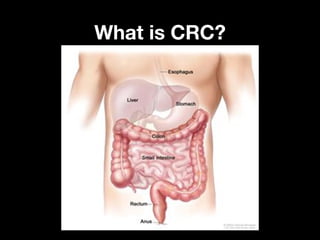
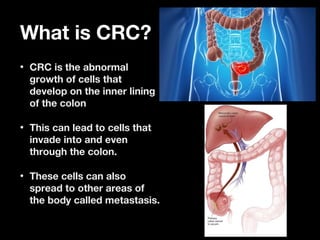

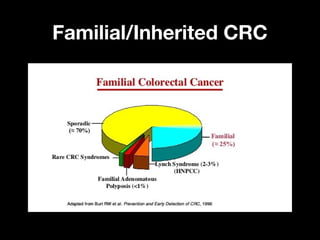
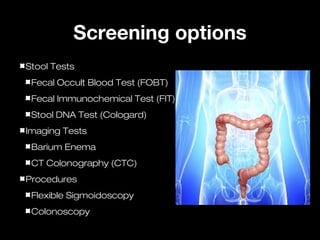
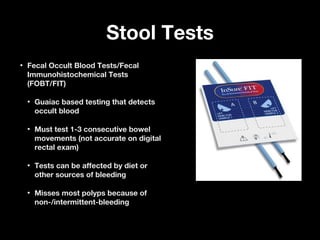


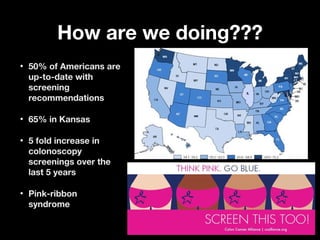

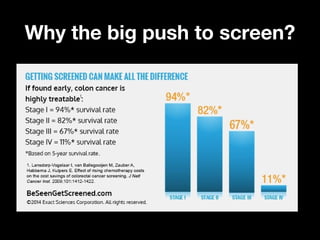

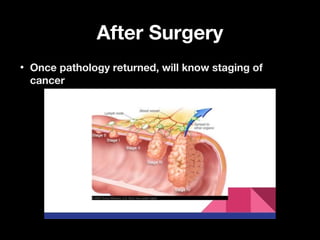



This document discusses colon cancer screening and prevention. It begins by stating that colon cancer is the third most common cancer in the US, with a lifetime risk of about 5%. Several risk factors are identified, including age, race, diet, obesity, tobacco and alcohol use, and family history. Screening options like stool tests, imaging tests, sigmoidoscopy, and colonoscopy are described. Colonoscopy is emphasized as the most sensitive screening method, allowing detection and removal of polyps. Guidelines recommend annual stool tests, sigmoidoscopy every 5 years, or colonoscopy every 10 years for average risk individuals starting at age 50. Earlier and more frequent screening is advised for those with family histories of colon cancer. The document aims to encourage screening and



























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














