Download as PDF, PPTX
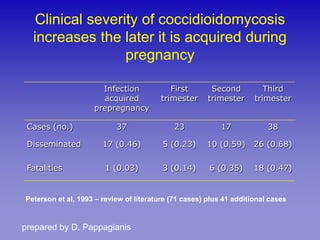

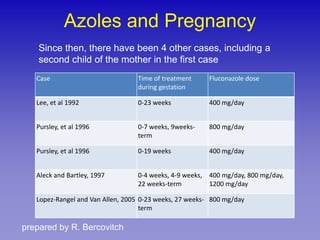
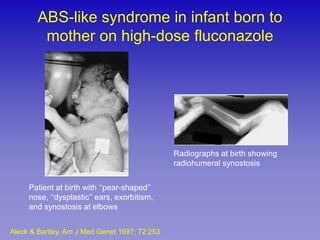



This document discusses coccidioidomycosis (Valley fever) during pregnancy. It notes that the infection is more severe when acquired during pregnancy, especially in the third trimester, and that the use of azole antifungals during pregnancy can be teratogenic. It reviews literature on cases of coccidioidomycosis in pregnancy and the effect of sex hormones on fungal growth. It also discusses the risk of birth defects from azole exposure during pregnancy, specifically the Antley-Bixler syndrome. The document provides recommendations for managing coccidioidomycosis in pregnant women based on their infection status and trimester.











































































































