Downloaded 19 times
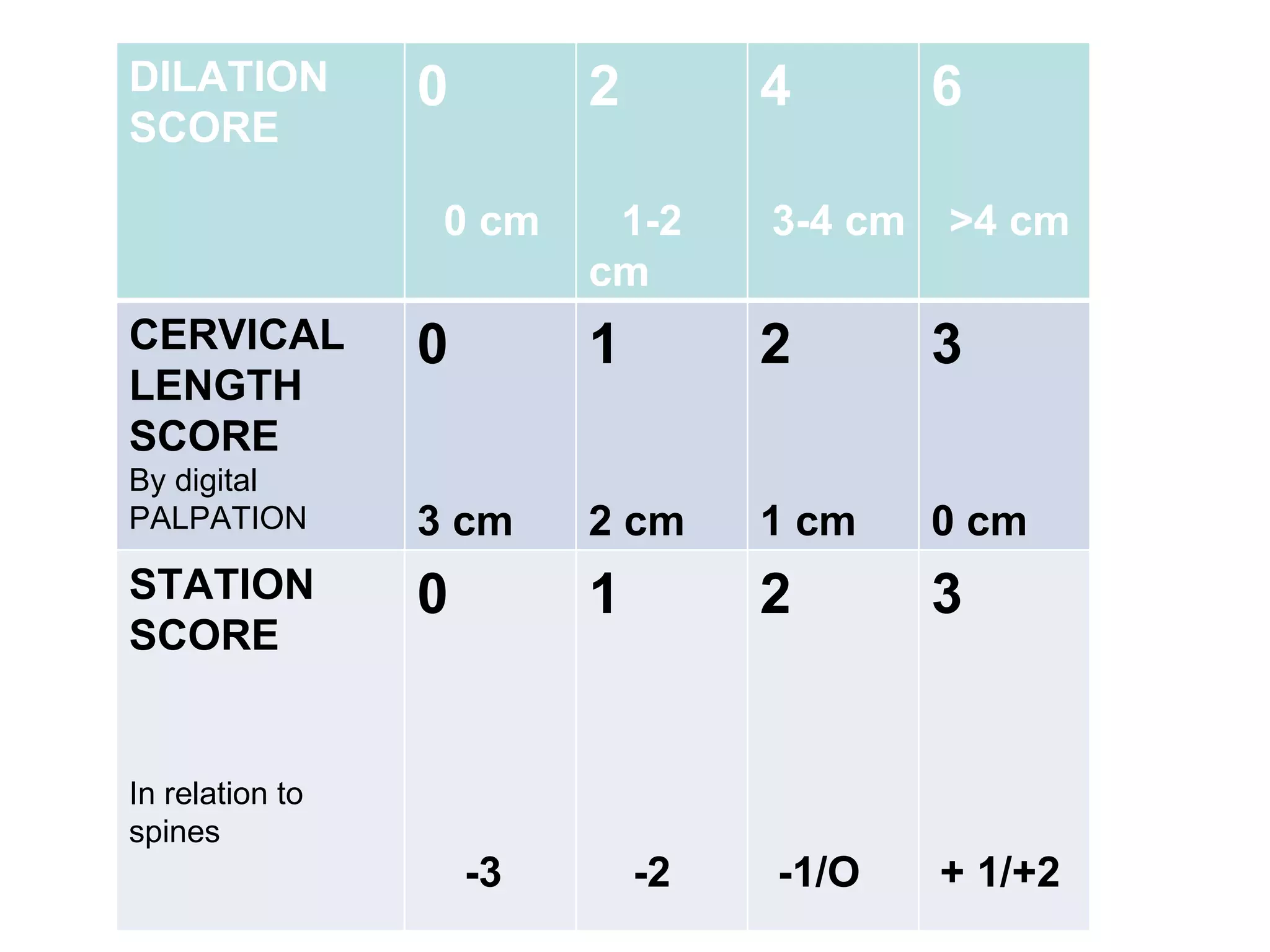
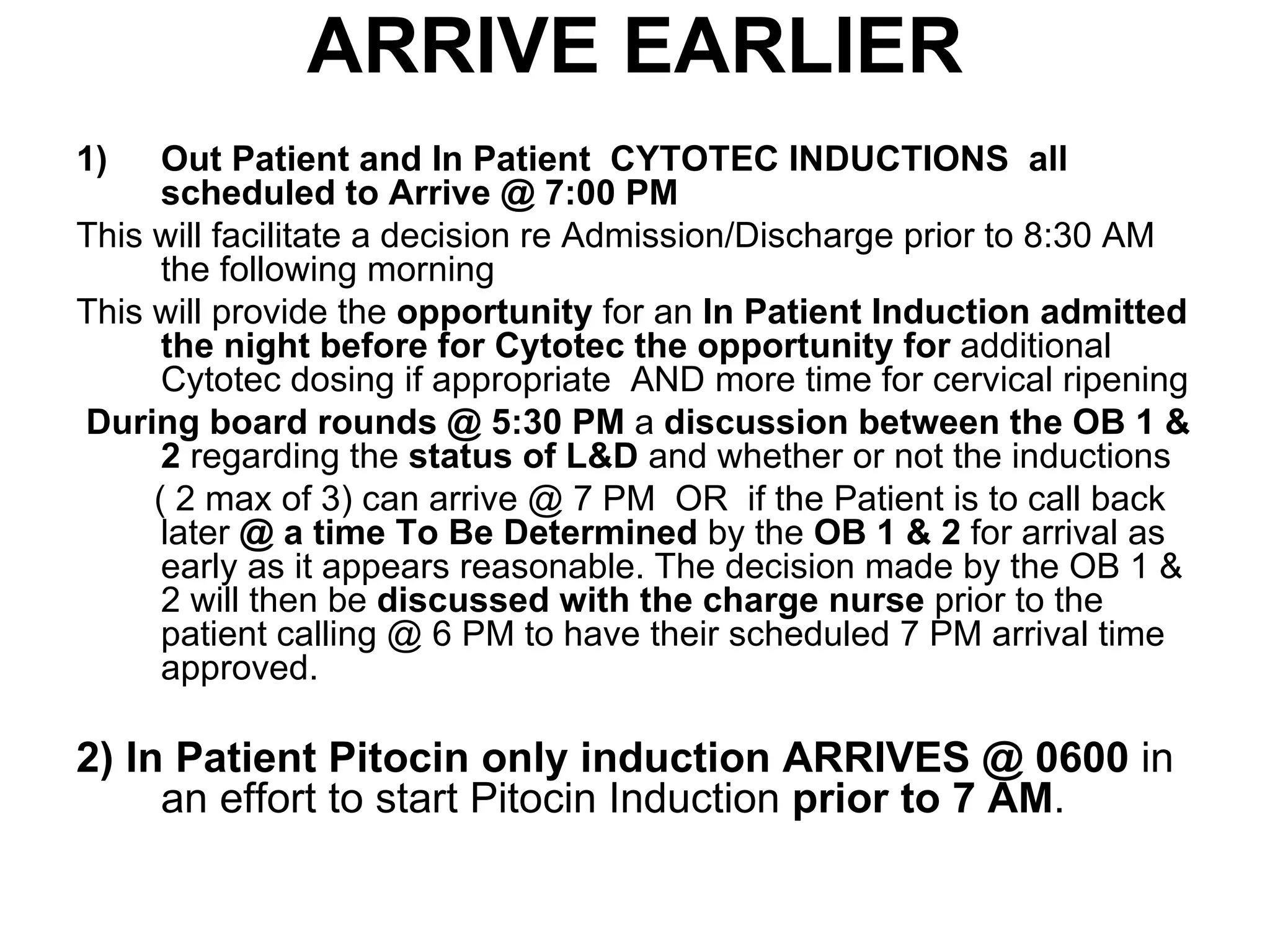
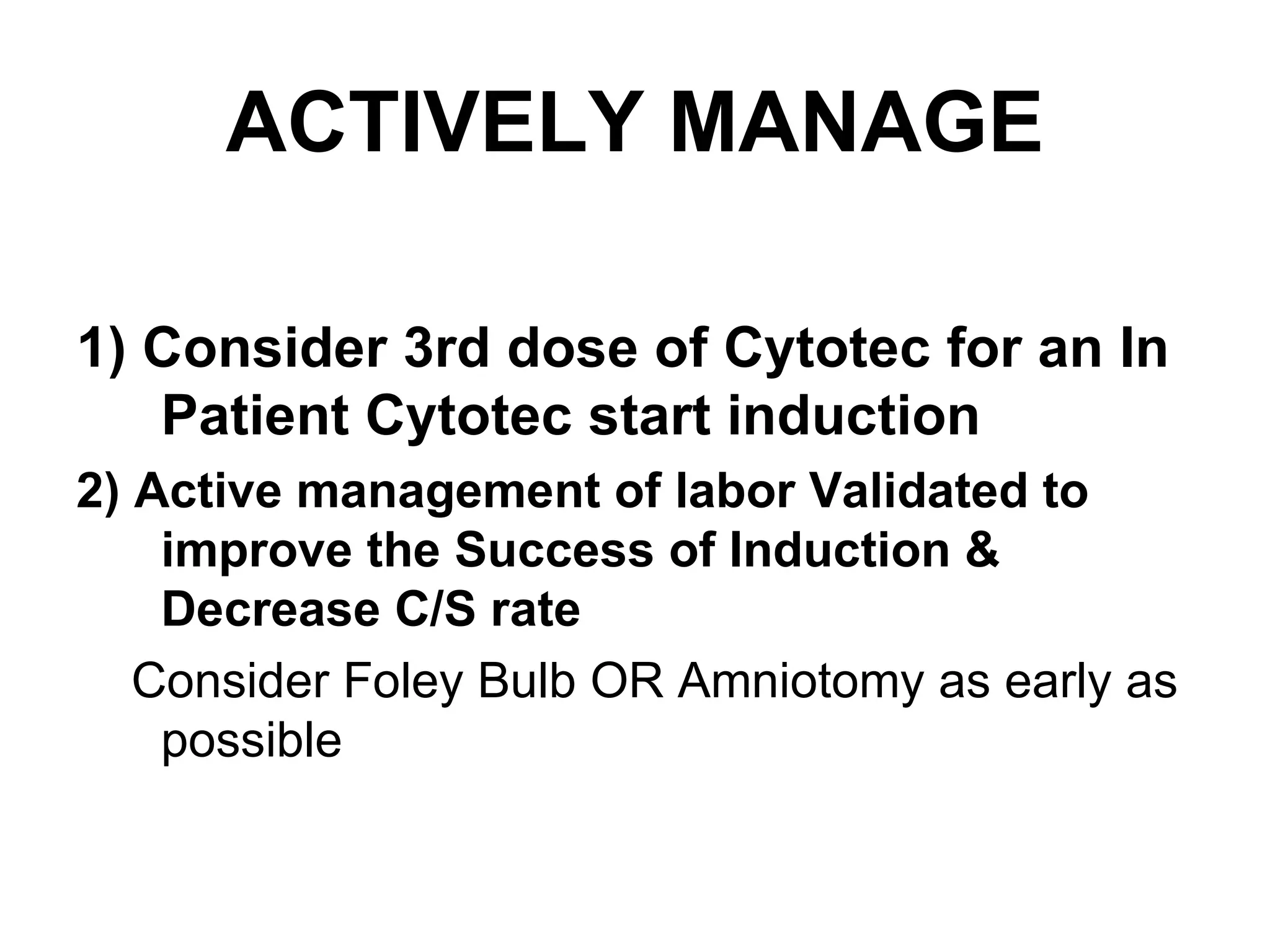

This document provides guidelines for induction of labor, including: 1. Recommending inpatient and outpatient Cytotec inductions arrive at 7:00 PM to facilitate admission/discharge decisions and additional Cytotec doses if needed. 2. Inpatient Pitocin-only inductions should arrive at 6:00 AM to start Pitocin before 7:00 AM. 3. Favorable criteria for induction include a modified Bishop score of 6 or more and cervical dilation of 3-4 cm for nulliparous patients.



































































