Download as PDF, PPTX

![2. Amniocentesis
should not be performed before the skin lesions
have completely healed.
may be performed to confirm the diagnosis with
PCR identification of VZV DNA.
In the absence of ultra-sound scanning finding
positive amniocentesis has a high sensitivity
but low specificity for the development of VZV.
If the PCR is positive but the ultrasound normal at
17-21 w
risk of FVS is low
if repeat ultrasound scanning at 24 w is also
normal then the risk of FVS is almost zero.
The risk, conversely, is very high if there are
ultrasound features and positive PCR [D].ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/chickenpox-180624212540/85/Chickenpox-in-pregnancy-31-320.jpg)
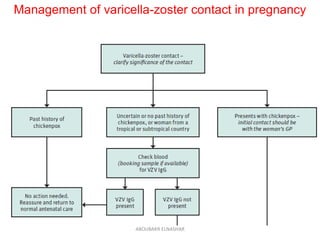
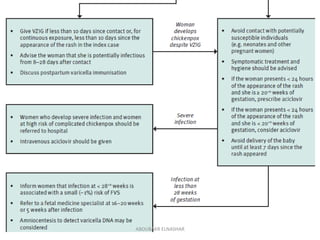

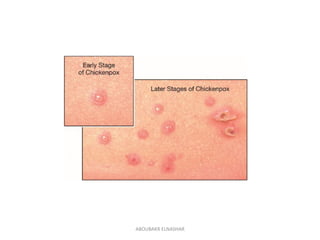
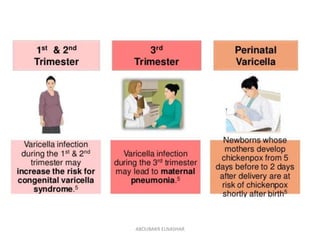
This document discusses chickenpox (varicella) infection during pregnancy. It notes that varicella poses risks to both the mother and fetus, with fetal risks being highest between 13-28 weeks gestation when it can cause fetal varicella syndrome. For pregnant women exposed to chickenpox, VZIG immunoglobulin within 10 days of exposure can reduce risks if she is not already immune. Developing chickenpox during pregnancy requires symptomatic treatment and potentially aciclovir. Risks to the newborn are highest if the mother develops chickenpox shortly before delivery.























































































