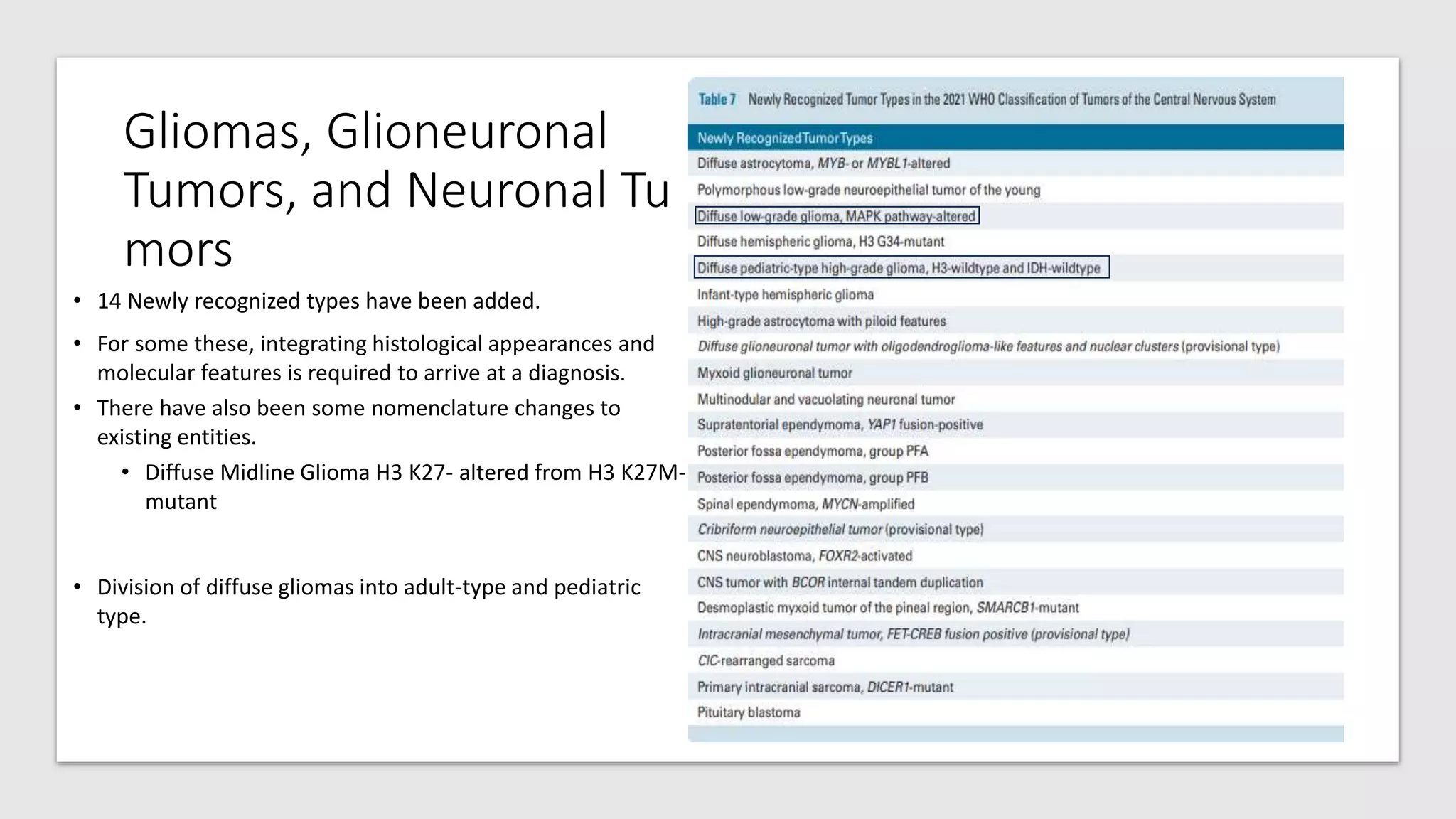
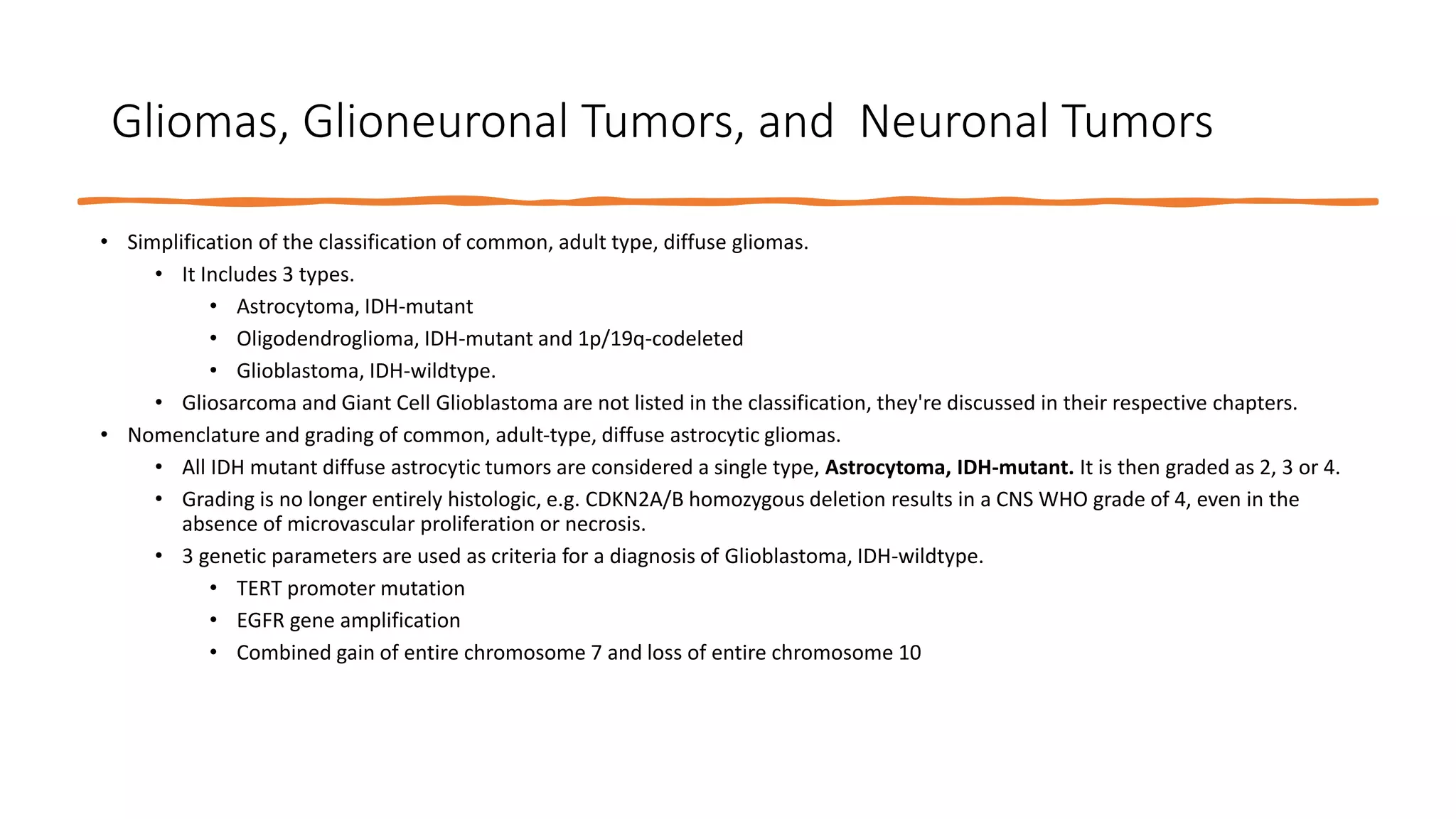
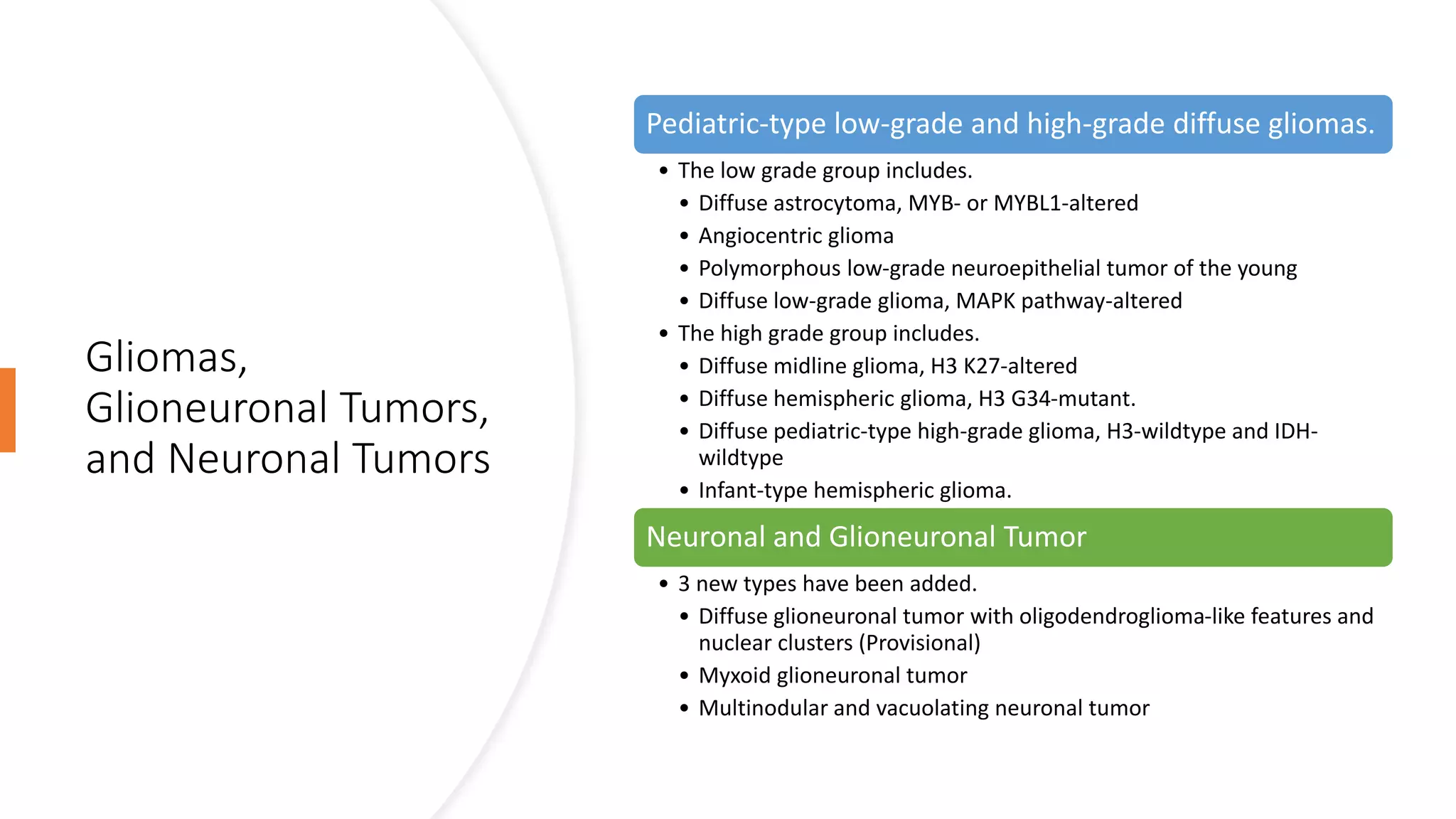
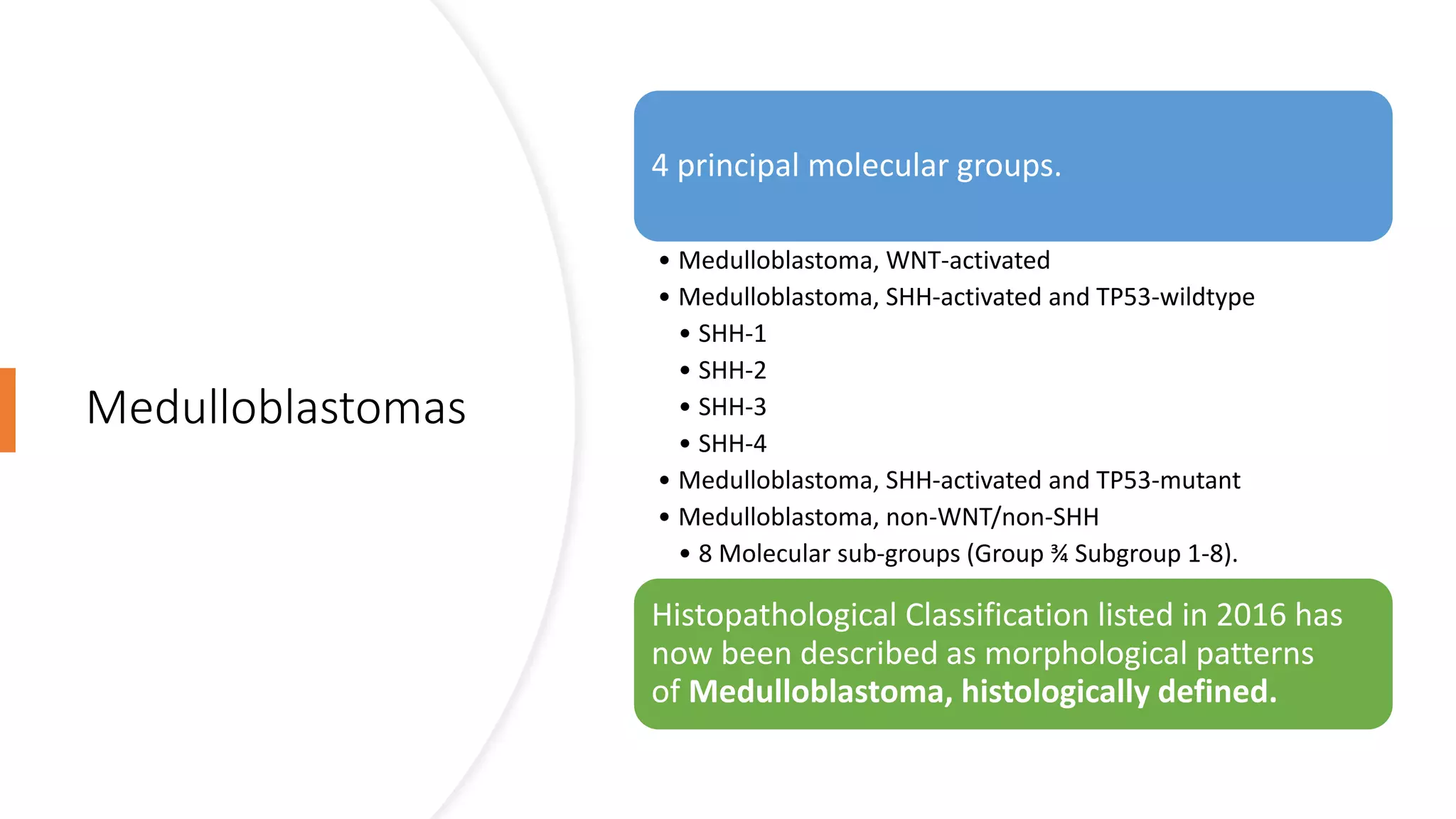
The document outlines the 2021 WHO classification of central nervous system (CNS) tumors, highlighting significant changes in tumor taxonomy, genetic associations, and the introduction of molecular parameters for more accurate diagnoses. It details the grouping of tumors based on genetic alterations, simplification of nomenclature, and the use of new grading systems that incorporate molecular features as biomarkers for prognosis. Additionally, the classification now includes various CNS tumor types, emphasizes integrated diagnoses, and updates the diagnostic technologies used in CNS tumor classification.