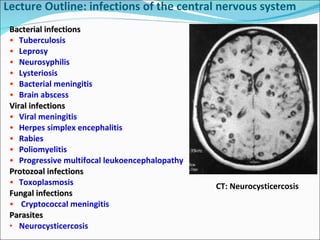
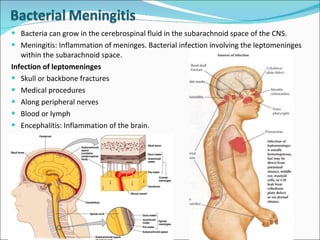
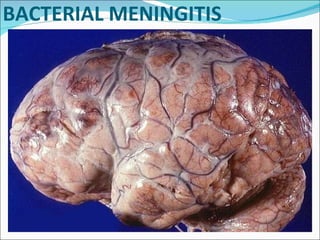
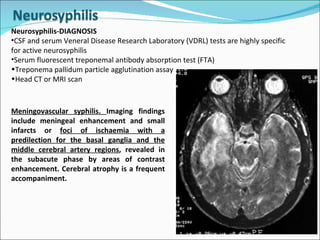
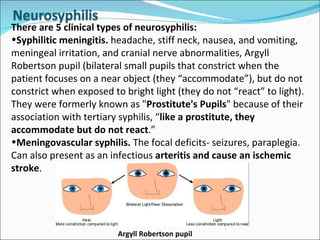
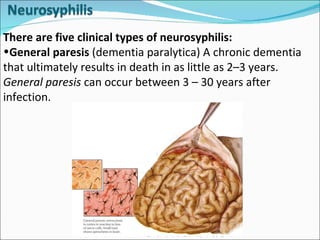
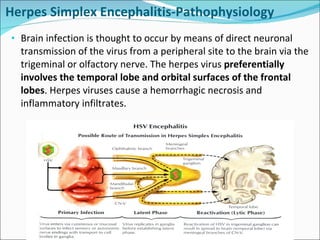
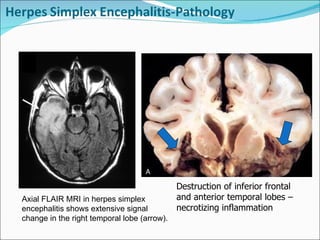
This document provides an overview of various infections that can affect the central nervous system, including bacteria, viruses, parasites, and fungi. It discusses specific conditions like bacterial meningitis, neurosyphilis, herpes simplex encephalitis, poliomyelitis, rabies, and more. For each, it covers topics like causes, clinical manifestations, diagnosis, treatment and prognosis.