
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Charcot-Marie-Tooth disease
Similar to Charcot-Marie-Tooth disease (20)
More from Vihari Rajaguru
More from Vihari Rajaguru (12)
Recently uploaded
Recently uploaded (20)
Charcot-Marie-Tooth disease
- 1. 1 | P a g e Kursk State Medical University The department of Biology, Medical Genetics and Ecology Head of the department: Prof. A.P.Ivanov Teacher in charge : Prof. V.A. Polonikov Topic : Charcot-Marie-Tooth disease Name : Vihari Vichakshana Rajaguru Group : No 32 Year : 4th year 2nd semester (2016)
- 2. 2 | P a g e What is Charcot-Marie-Tooth disease? Charcot-Marie-Tooth disease (CMT) is one of the most common inherited neurological disorders, affecting approximately 1 in 2,500 people in the United States. The disease is named for the three physicians who first identified it in 1886 - Jean-Martin Charcot and Pierre Marie in Paris, France, and Howard Henry Tooth in Cambridge, England. CMT, also known as hereditary motor and sensory neuropathy (HMSN) or peroneal muscular atrophy, comprises a group of disorders that affect peripheral nerves. The peripheral nerves lie outside the brain and spinal cord and supply the muscles and sensory organs in the limbs. Disorders that affect the peripheral nerves are called peripheral neuropathies.
- 3. 3 | P a g e History The disease is named after those who classically described it: Jean- Martin Charcot (1825–1893), his pupil Pierre Marie(1853–1940) ("Sur une forme particulière d'atrophie musculaire progressive, souvent familiale débutant par les pieds et les jambes et atteignant plus tard les mains". Revue médicale. Paris. 6: 97–138. 1886.), and Howard Henry Tooth (1856–1925) ("The peroneal type of progressive muscular atrophy", dissertation, London, 1886.) Jean Martin Charcot What are the symptoms of Charcot-Marie- Tooth disease? The neuropathy of CMT affects both motor and sensory nerves. (Motor nerves cause muscles to contract and control voluntary muscle activity such as speaking, walking, breathing, and swallowing.) A typical feature includes weakness of the foot and lower leg muscles, which may result in foot drop and a high-stepped gait with frequent tripping or falls. Foot deformities, such as high arches and hammertoes (a condition in which the middle joint of a toe bends upwards) are also characteristic due to weakness of the small muscles in the feet. In addition, the lower legs may take on an "inverted champagne bottle" appearance due to the loss of muscle bulk. Later in the disease, weakness and muscle atrophy may occur in the hands, resulting in
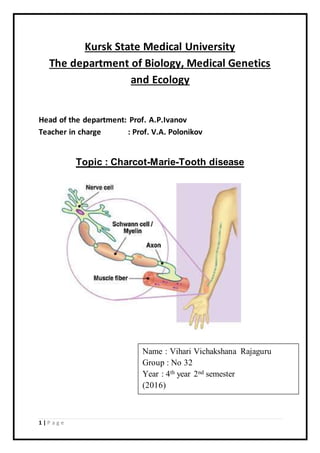
- 4. 4 | P a g e difficulty with carrying out fine motor skills (the coordination of small movements usually in the fingers, hands, wrists, feet, and tongue). Onset of symptoms is most often in adolescence or early adulthood, but some individuals develop symptoms in mid-adulthood. The severity of symptoms varies greatly among individuals and even among family members with the disease. Progression of symptoms is gradual. Pain can range from mild to severe, and some people may need to rely on foot or leg braces or other orthopedic devices to maintain mobility. Although in rare cases, individuals may have respiratory muscle weakness, CMT is not considered a fatal disease and people with most forms of CMT have a normal life expectancy. What causes Charcot-Marie-Tooth disease? A nerve cell communicates information to distant targets by sending electrical signals down a long, thin part of the cell called the axon. In order to increase the speed at which these electrical signals travel, the axon is insulated by myelin, which is produced by another type of cell called the Schwann cell. Myelin twists around the axon like a jelly-roll cake and prevents the loss of electrical signals.
- 5. 5 | P a g e Without an intact axon and myelin sheath, peripheral nerve cells are unable to activate target muscles or relay sensory information from the limbs back to the brain. CMT is caused by mutations in genes that produce proteins involved in the structure and function of either the peripheral nerve axon or the myelin sheath. Although different proteins are abnormal in different forms of CMT disease, all of the mutations affect the normal function of the peripheral nerves. Consequently, these nerves slowly degenerate and lose the ability to communicate with their distant targets. The degeneration of motor nerves results in muscle weakness and atrophy in the extremities (arms, legs, hands, or feet), and in some cases the degeneration of sensory nerves results in a reduced ability to feel heat, cold, and pain. The gene mutations in CMT disease are usually inherited. Each of us normally possesses two copies of every gene, one inherited from each parent. Some forms of CMT are inherited in an autosomal dominant fashion, which means that only one copy of the abnormal gene is needed to cause the disease. Other forms of CMT are inherited in an autosomal recessive fashion, which means that both copies of the abnormal gene must be present to cause the disease. Still other forms of CMT are inherited in an X-linked fashion, which means that the abnormal gene is located on the X chromosome.The X and Y chromosomes determine an individual's sex. Individuals with two X chromosomes are female and individuals with one X and one Y chromosome are male. In rare cases the gene mutation causing CMT disease is a new mutation which occurs spontaneously in the individual's genetic material and has not been passed down through the family. Is there a gene implicated in Charcot-Marie- Tooth? The newly discovered GARS gene (see Gene Discovery Opens Door to FurtherResearch In InheritedNeurologicalDisorders [News Release]) is implicated in CMT type 2D, a form of CMT that primarily affects the
- 6. 6 | P a g e hands and the forearms. CMT type 2D is inherited in an autosomal dominant fashion. Even though the GARS gene is implicated in only two specific types of CMT, this discovery will guide researchers in studying other forms of these diseases, as well as other neurological disorders. Because carpal tunnel syndrome affects the hands and the forearms, scientists may now investigate whether the GARS gene plays some role in this disorder. And two defective forms of the gene implicated in Lou Gehrig's disease are known to interact with a GARS family member. Ultimately, the GARS gene and its family may provide a rich new resource for scientists investigating inherited and non-inherited neurological diseases. What are the types of Charcot-Marie-Tooth disease? There are many forms of CMT disease, including CMT1, CMT2, CMT3, CMT4, and CMTX. CMT1,caused by abnormalities in the myelin sheath, has three main types. CMT1A is an autosomal dominant disease that results from a duplication of the gene on chromosome 17 that carries the instructions for producing the peripheral myelin protein-22 (PMP-22). The PMP-22 protein is a critical component of the myelin sheath. Overexpression of this gene causes the structure and function of the myelin sheath to be abnormal.
- 7. 7 | P a g e Patients experience weakness and atrophy of the muscles of the lower legs beginning in adolescence; later they experience hand weakness and sensory loss. Interestingly, a different neuropathy distinct from CMT1A called hereditary neuropathy with predisposition to pressure palsy (HNPP) is caused by a deletion of one of the PMP-22 genes. In this case, abnormally low levels of the PMP-22 gene result in episodic, recurrent demyelinating neuropathy. CMT1B is an autosomal dominant disease caused by mutations in the gene that carries the instructions for manufacturing the myelin protein zero (P0), which is another critical component of the myelin sheath. Most of these mutations are point mutations, meaning a mistake occurs in only one letter of the DNA genetic code. To date, scientists have identified more than 120 different point mutations in the P0 gene. As a result of abnormalities in P0, CMT1B produces symptoms similar to those found in CMT1A. The less common CMT1C, CMT1D, and CMT1E, which also have symptoms similar to those found in CMT1A, are caused by mutations in the LITAF, EGR2, and NEFL genes, respectively. CMT2 results from abnormalities in the axon of the peripheral nerve cell rather than the myelin sheath. It is less common than CMT1. CMT2A, the most common axonal form of CMT, is caused by mutations in Mitofusin 2, a protein associated with mitochondrial fusion. CMT2A has also been linked to mutations in the gene that codes for the kinesin family member 1B-beta protein, but this has not been replicated in other cases. Kinesins are proteins that act as motors to help power the transport of materials along the cell. Other less common forms of CMT2 have been recently identified and are associated with various
- 8. 8 | P a g e genes: CMT2B (associated with RAB7), CMT2D (GARS). CMT2E (NEFL), CMT2H (HSP27), and CMT2l (HSP22). CMT3 or Dejerine-Sottas disease is a severe demyelinating neuropathy that begins in infancy. Infants have severe muscle atrophy, weakness, and sensoryproblems.This rare disordercan be caused by a specific point mutation in the P0 gene or a point mutation in the PMP-22 gene. CMT Type Chromosome; Inheritance Pattern Age of Onset Clinical Features Average NCVs§ CMT 1A (PMP- 22¶ dupl.) 17p11; AD* First decade Distal weakness 15-20 m/s CMT 1B (P0 - MPZ)** 1q22; AD First decade Distal weakness <20 m/s CMT 1C (non A, non B) 16p13;AD Second decade Distal weakness 26-42 m/s CMT 1D (early growth response [EGR]–2 10q21; AD First decade Distal weakness 15-20 m/s CMT 1E 17p11; AD First decade Distal weakness, deafness 15-20 m/s CMT 1F 8p21; AD First decade Distal weakness 15-20 m/s CMT X (Connexin-32) Xq13; XD‡ Second decade Distal weakness 25-40 m/s CMT 2A 1p36; AD 10 y Distal weakness >38 m/s CMT 2B 3q; AD Second decade Distal weakness, sensory loss, skin ulcers Axon loss; Normal Table 1. Charcot-Marie-Tooth Disorders: Genetic and ClinicalFeature Comparison
- 9. 9 | P a g e CMT 2C 12q23-q24, AD First decade Vocal cord, diaphragm, and distal weakness >50 m/s CMT 2D 7p14; AD 16-30 y Distal weakness, upper limb predominantly Axon loss; N†† CMT 2E 8p21; AD 10-30 y Distal weakness, lower limb predominantly Axon loss; N CMT 2F 7q11-q21; AD 15-25 y Distal weakness Axon loss; N CMT 2G 12q12-q13; ?AD 9-76 y Distal weakness Axon loss; N CMT 2H ?; AR† 15-25 y Distal weakness, Pyramidal features Axon loss; N CMT 2I 1q22; AD 47-60 y Distal weakness Axon loss; N CMT 2J 1q22; AD 40-50 y Distal weakness, hearing loss Axon loss; N CMT 2K 8q13-q21; AR <4 y Distal weakness Axon loss; N CMT 2L 12q24; AD 15-25 y Distal weakness Axon loss; N CMT R-Ax (Ouvrier) AR First decade Distal weakness Axon loss; N CMT R-Ax (Moroccan) 1q21; AR Second decade Distal weakness Axon loss; N
- 10. 10 | P a g e CMT4 comprises several different subtypes of autosomal recessive demyelinating motor and sensory neuropathies. Each neuropathy subtype is caused by a different genetic mutation, may affect a particular ethnic population, and produces distinct physiologic or clinical characteristics. Individuals with CMT4 generally develop symptoms of leg weakness in childhood and by adolescence they may not be able to walk. Several genes have been identified as causing CMT4, including GDAP1 (CMT4A), MTMR13 (CMT4B1), MTMR2 (CMT4B2), SH3TC2 (CMT4C), NDG1 (CMT4D), EGR2 (CMT4E), PRX (CMT4F), FDG4 (CMT4H), and FIG4 (CMT4J). CMTX is caused by a point mutation in the connexin-32 gene on the X chromosome. The connexin-32 protein is expressed in Schwann cells- cells that wrap around nerve axons, making up a single segment of the myelin sheath. This protein may be involved in Schwann cell communication with the axon. Males who inherit one mutated gene from their mothers show moderate to severe symptoms of the disease Cowchock syndrome Xq24-q26 First decade Distal weakness, deafness, mental retardation Axon loss; N HNPP|| (PMP-22) Or tomaculous neuropathy 17p11; AD All ages Episodic weakness and numbness Conduction Blocks
- 11. 11 | P a g e beginning in late childhood or adolescence (the Y chromosome that males inherit from their fathers does not have the connexin-32 gene). Females who inherit one mutated gene from one parent and one normal gene from the other parent may develop mild symptoms in adolescence or later or may not develop symptoms of the disease at all. How is Charcot-Marie-Tooth disease diagnosed? Diagnosis of CMT begins with a standard medical history, family history, and neurological examination. Individuals will be asked about the nature and duration of their symptoms and whether other family members have the disease. During the neurologicalexamination a physician will look for evidence of muscle weakness in the individual's arms, legs, hands, and feet, decreased muscle bulk, reduced tendon reflexes, and sensory loss. Doctors look for evidence of foot deformities, such as high arches, hammertoes,inverted heel, or flat feet. Other orthopedic problems, such as mild scoliosis or hip dysplasia, may also be present. A specific sign that may be found in people with CMT1 is nerve enlargement that may be felt or even seen through the skin. These enlarged nerves, called hypertrophic nerves, are caused by abnormally thickened myelin sheaths. If CMT is suspected, the physician may order electrodiagnostic tests. This testing consists of two parts: nerve conduction studies and electromyography (EMG). During nerve conduction studies, electrodes are placed on the skin over a peripheral motor or sensory nerve. These electrodes produce a small electric shock that may cause mild discomfort. This electrical impulse stimulates sensory and motor nerves and provides quantifiable information that the doctor can use to arrive at a diagnosis.EMG involves inserting a needle electrode through the skin to measure the bioelectrical activity of muscles. Specific abnormalities in the readings signify axon degeneration. EMG may be useful in further characterizing the distribution and severity of peripheral nerve involvement.
- 12. 12 | P a g e Genetic testing is available for some types of CMT and results are usually enough to confirm a diagnosis. In addition, genetic counseling is available to assist individuals in understanding their condition and plan for the future. If all the diagnostic work-up in inconclusive or genetic testing comes back negative, a neurologist may perform a nerve biopsy to confirm the diagnosis. A nerve biopsyinvolves removing a small piece of peripheral nerve through an incision in the skin. This is most often done by removing a piece of the nerve that runs down the calf of the leg. The nerve is then examined under a microscope. Individuals with CMT1 typically show signs of abnormal myelination. Specifically, "onion bulb" formations may be seen which represent axons surrounded by layers of demyelinating and remyelinating Schwann cells. Individuals with CMT1 usually show signs of axon degeneration. Recently, skin biopsy has been used to study unmyelinated and myelinated nerve fibers in a minimally invasive way, but their clinical use in CMT has not yet been established. Diagnostic Considerations In addition to the conditions listed in the differential diagnosis,other problems to be consideredinclude the following: Acquired nongenetic causes of peripheral neuropathies Vitamin B12 deficiency Thyroid disease Diabetes mellitus Vasculitis Amyloid associated with chronic inflammation Occult malignancy Heavy-metal intoxication Chronic inflammatory demyelinating polyneuropathy Motor neuropathy with multiple conductionblock Other genetic neuropathies Familial brachial plexus neuropathy (ie, hereditary neuralgic amyotrophy) Autosomalrecessive genetic disorders,such as Refsum disease or metachromatic leukodystrophy
- 13. 13 | P a g e X-linked recessive genetic disorders,such as adrenomyeloneuropathy or Pelizaeus-Merzbacher disease Amyloid neuropathies Hereditary ataxias with neuropathy (eg, Friedreichataxia) Blindness,seizures, dementia, and mental retardation are not part of Charcot-Marie-Tooth syndrome. Differential Diagnoses Alcoholism Leprosy Neurosyphilis Pediatric HIV Infection How is Charcot-Marie-Tooth disease treated? There is no cure for CMT, but physical therapy, occupational therapy, braces and other orthopedic devices, and even orthopedic surgery can help individuals cope with the disabling symptoms of the disease. In addition, pain-killing drugs can be prescribed for individuals who have severe pain. Physical and occupational therapy, the preferred treatment for CMT, involves muscle strength training, muscle and ligament stretching, stamina training, and moderate aerobic exercise. Most therapists recommend a specialized treatment program designed with the approval of the person's physician to fit individual abilities and needs. Therapists also suggest entering into a treatment program early; muscle strengthening may delay or reduce muscle atrophy, so strength training is most useful if it begins before nerve degeneration and muscle weakness progress to the point of disability. Stretching may prevent or reduce joint deformities that result from uneven muscle pull on bones. Exercises to help build stamina or increase endurance will help prevent the fatigue that results from performing everyday activities that require strength and mobility. Moderate aerobic activity can help to maintain cardiovascular fitness and overall health. Most therapists recommend low-impact or no-impact exercises, such as biking or swimming, rather than activities such as walking or jogging, which may put stress on fragile muscles and joints.
- 14. 14 | P a g e Many CMT patients require ankle braces and other orthopedic devices to maintain everyday mobility and prevent injury. Ankle braces can help prevent ankle sprains by providing support and stability during activities such as walking or climbing stairs. High-top shoes or boots can also provide support for weak ankles. Thumb splints can help with hand weakness and loss of fine motor skills. Assistive devices should be used before disability sets in because the devices may prevent muscle strain and reduce muscle weakening. Some individuals with CMT may decide to have orthopedic surgery to reverse foot and joint deformities. Prognosis The severity of symptoms vary widely even for the same type of CMT. There have been cases of monozygotic twins with varying levels of disease severity, showing that identical genotypes are associated with differentlevels of severity some patients are able to live a normal life and are almost or entirely asymptomatic. A 2007 review stated that "Life expectancy is not known to be altered in the majority of cases. What research is being done? The NINDS supports research on CMT and other peripheral neuropathies in an effort to learn how to better treat, prevent, and even cure these disorders.Ongoing research includes efforts to identify more of the mutant genes and proteins that cause the various disease subtypes,efforts to discoverthe mechanisms of nerve degeneration and muscle atrophy with the hope of developing interventions to stop or slow down these debilitating processes, and efforts to find therapies to reverse nerve degeneration and muscle atrophy. One promising area of research involves gene therapy experiments. Research with cell cultures and animal models has shown that it is possible to deliver genes to Schwann cells and muscle. Another area of research involves the use of trophic factors or nerve growth factors, such as the hormone androgen, to prevent nerve degeneration. Vitamin C has been studied in CMT1A and the results of a multicentric trial are due soon. Curcumin, a component of curry, is currently being studied as a treatment strategy in an animal model of CMT1B.
- 15. 15 | P a g e Research helps us better understand diseases and can lead to advances in diagnosis and treatment. This sectionprovides resources to help you learn about medical research and ways to get involved. Clinical Research Resources ClinicalTrials.gov lists trials that are studying or have studied Charcot- Marie-Tooth disease. Click on the link to go to ClinicalTrials.gov to read descriptions of these studies. The Research Portfolio Online Reporting Tool (RePORT) provides access to reports, data, and analyses of research activities at the National Institutes of Health (NIH), including information on NIH expenditures and the results of NIH-supported research. Although these projects may not conduct studies on humans, you may want to contact the investigators to learn more. To search for studies, enter the disease name in the "Text Search" box. Then click "Submit Query". Patient Registry The Inherited Neuropathies Consortium is a team of doctors, nurses, research coordinators, and research labs throughout the U.S., working together to improve the lives of people with Charcot Marie Tooth disease through research. The Inherited Neuropathies Consortium has a registry for patients who wish to be contacted about clinical research opportunities.
- 16. 16 | P a g e References 1. Charcot-Marie-Tooth Disease. MedlinePlus. 2016; http://www.nlm.nih.gov/medlineplus/ency/article/000 727.htm. 2. Charcot-Marie-Tooth Fact Sheet. National Institute of Neurological Disorders and Stroke (NINDS). 2016; http://www.ninds.nih.gov/disorders/charcot_marie_to oth/detail_charcot_marie_tooth.htm#102833092. 3. eMedicine Journal [emedicine.medscape.com] There are two articles by Divakara Kedlaya, MBBS, Associate Professor, Department of Physical Medicine and Rehabilitation, Loma Linda University Medical Center, about Charcot-Marie-Tooth Disease at the eMedicine Journal website. One last updated in September 2012 and another last updated on May 2012 4. http://emedicine.medscape.com/article/1173484-overview 5. https://en.wikipedia.org/wiki/Charcot%E2%80%93Marie%E 2%80%93Tooth_disease 6. Physical Medicine and Rehabilitation for Charcot-Marie-Tooth Disease. Medscape. Retrieved March 20, 2012.