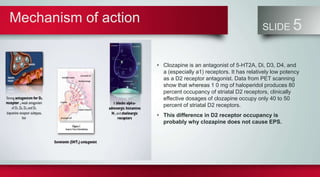
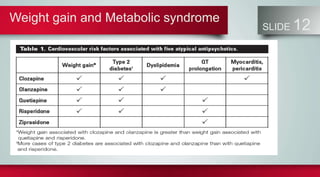
Clozapine is an atypical antipsychotic that is used for treatment-resistant schizophrenia and other psychotic disorders. It works by antagonizing serotonin, dopamine, and other receptors with relatively low potency for the D2 receptor. This allows it to be effective without causing extrapyramidal side effects. Clozapine has indications for treatment-resistant schizophrenia, tardive dyskinesia, mania, and others. It requires monitoring of white blood cell counts due to the risk of agranulocytosis. Common side effects include sedation, dizziness, tachycardia, nausea, and weight gain.