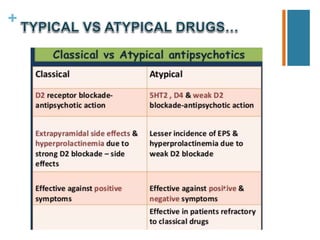
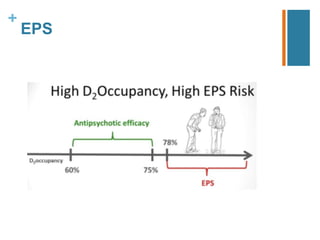
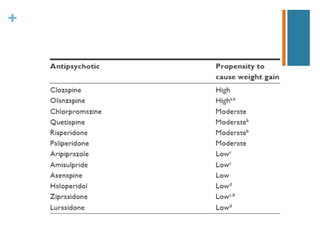
Second-generation antipsychotics have fewer extrapyramidal side effects than first-generation drugs. They include risperidone, paliperidone, olanzapine, quetiapine, ziprasidone, aripiprazole, asenapine, iloperidone, lurasidone, and clozapine. Clozapine is reserved for treatment-resistant cases due to its risk of agranulocytosis. These drugs differ in their receptor binding profiles and side effect risks like weight gain, metabolic effects, and QTc prolongation. Dosage selection depends on these factors and potential drug interactions.