The document summarizes key information about antipsychotic medications, including:
- There are two classes of antipsychotics: typical/conventional which block dopamine receptors and atypical/novel which block serotonin and dopamine receptors.
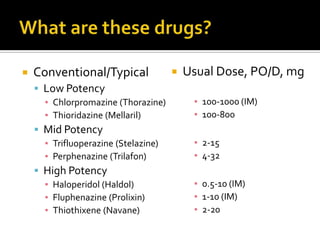
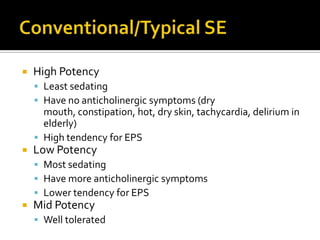
- Typical antipsychotics are further divided into low, mid, and high potency. High potency antipsychotics like haloperidol have the least sedation and anticholinergic side effects but highest risk of EPS.
- Atypical antipsychotics like clozapine, risperidone, and olanzapine tend not to cause EPS but can increase risks of weight gain, diabetes, and other side effects. Clozapine specifically requires regular blood