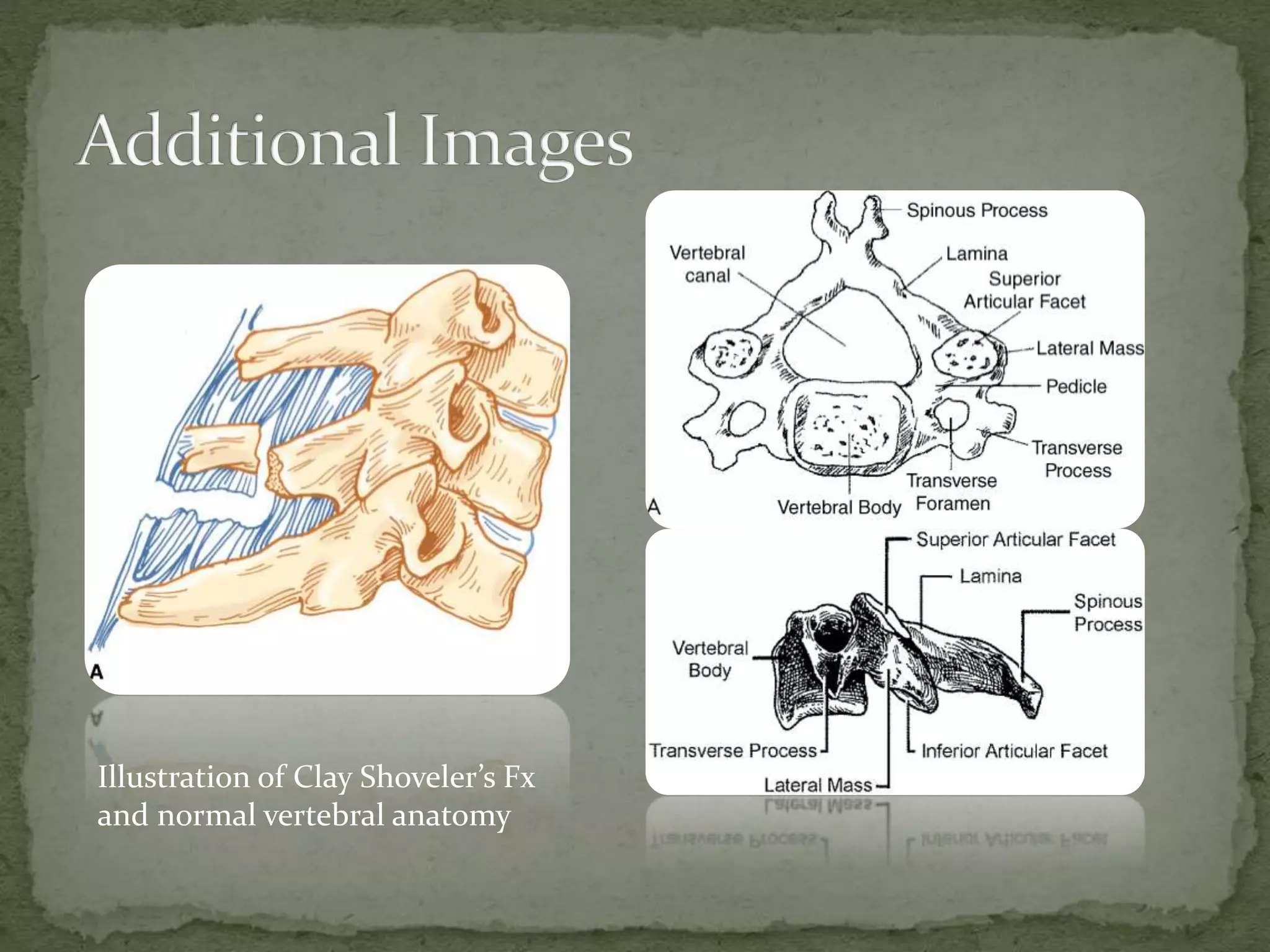
A 17-year-old male was involved in a head-on motor vehicle collision at 35-40 mph and presented with cervical neck pain but was ambulatory and alert. Imaging revealed a C6 spinous process fracture, known as a Clay Shoveler's fracture, which is considered stable and results from flexion against contracted neck muscles during deceleration. The patient was placed in a Philadelphia collar and advised to follow-up with orthopedics in 1-2 weeks for non-operative management given the isolated nature of the fracture.