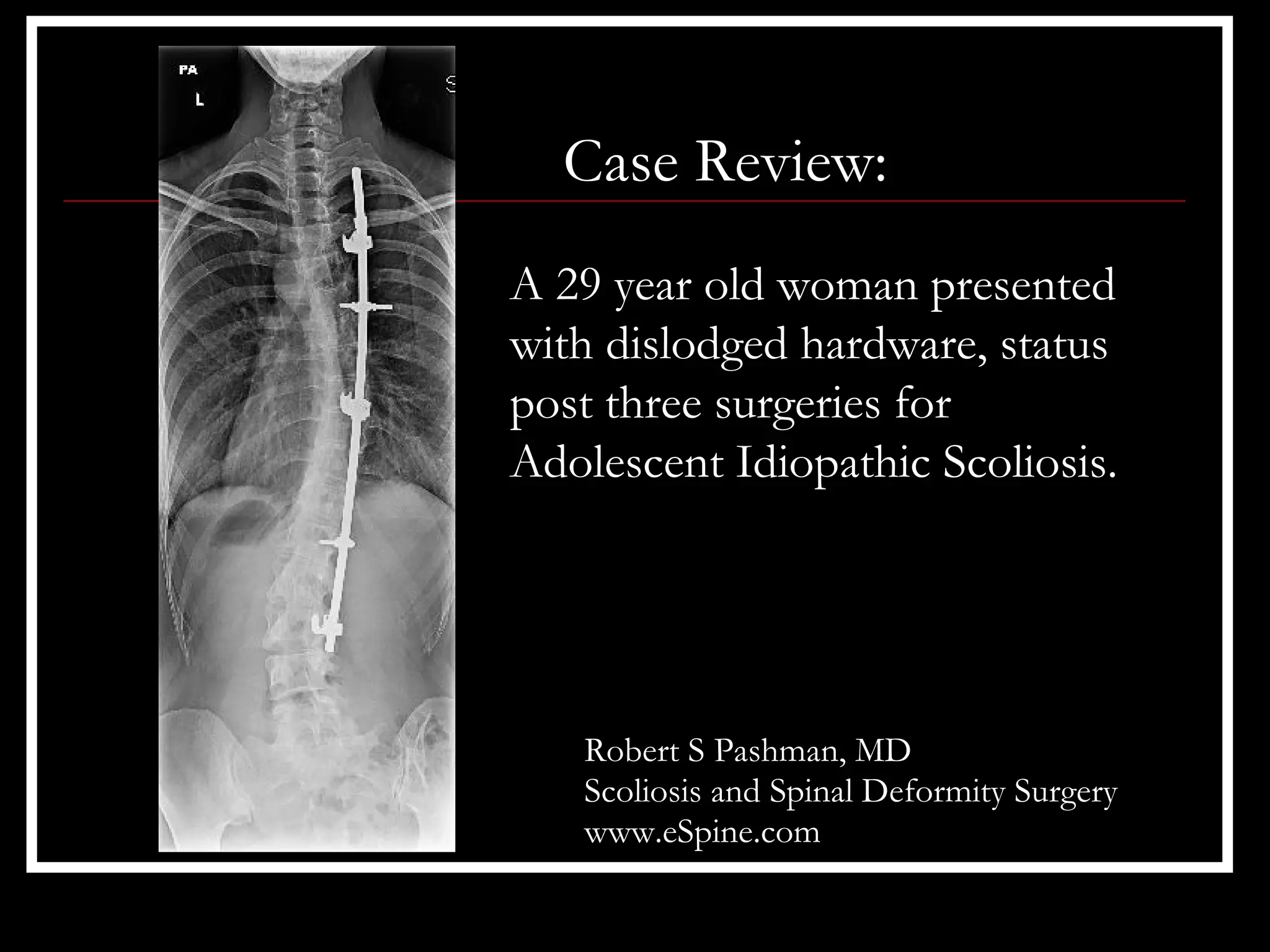
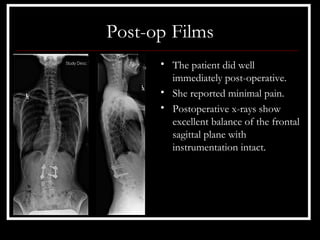
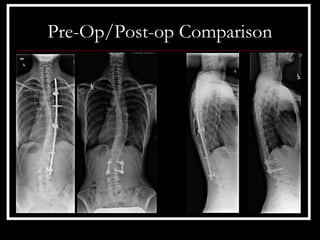

A 29-year old woman presented with dislodged hardware from three previous surgeries for adolescent idiopathic scoliosis. She had retained loose instrumentation from her past operations that posed a medical risk. The surgical strategy was to remove the retained hardware through osteotomies, perform spinal fusions from T4 to L3, and place new segmental instrumentation from L2 to L3.