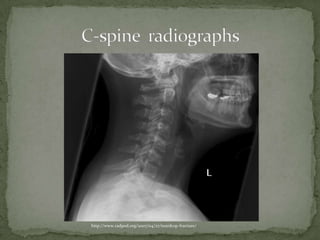
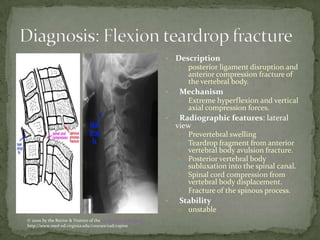
An 18 year old female presents to the emergency department with severe neck pain and weakness in her extremities after diving into a shallow pool while intoxicated. On examination, she has bruising on her face and tenderness in her neck with reduced strength and sensation below her arms. Radiographic images show features consistent with a teardrop fracture of her cervical spine, an unstable fracture caused by extreme neck flexion that results in spinal cord compression and requires spinal precautions, consultation, and possible admission.