Downloaded 692 times

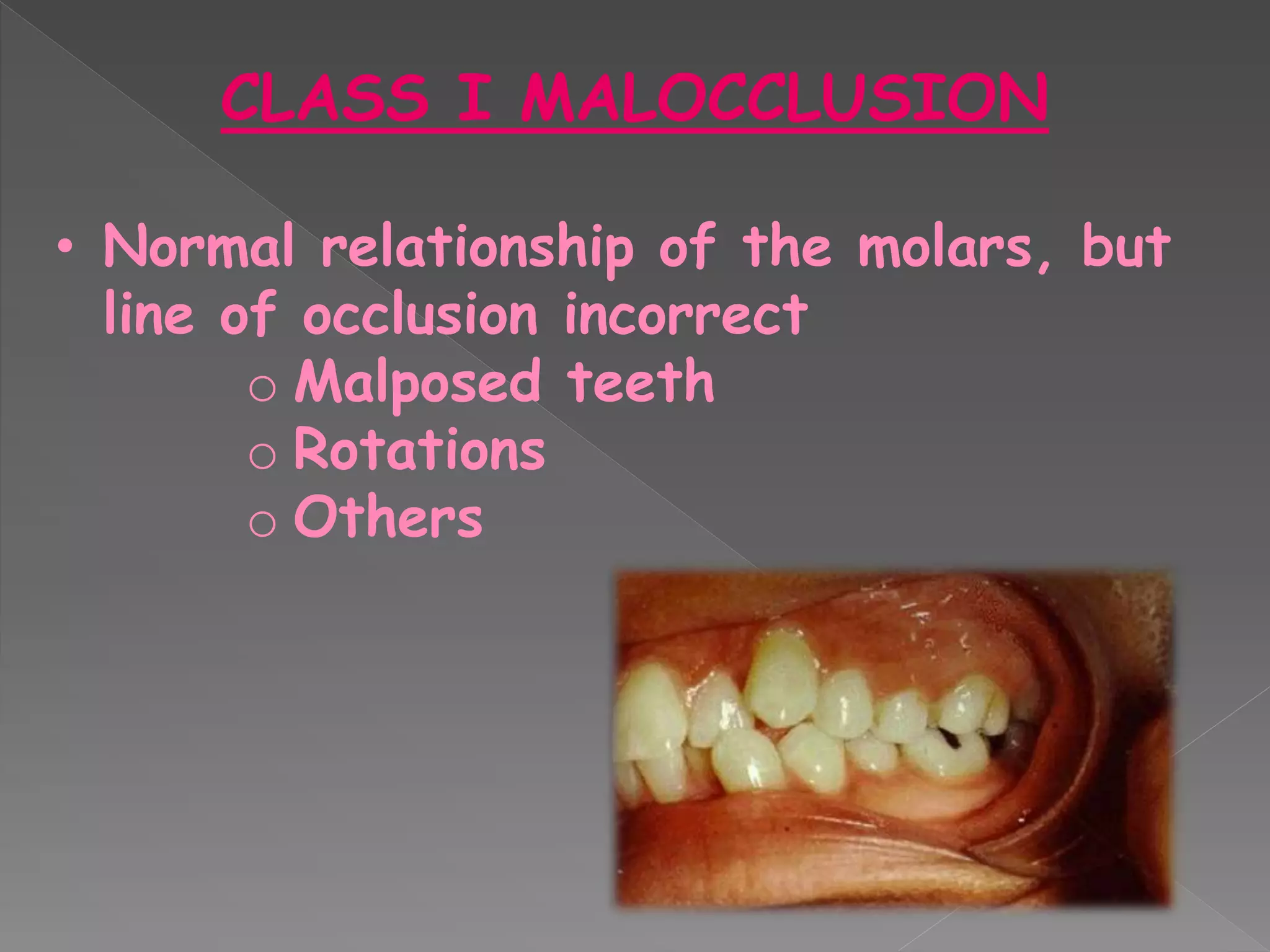
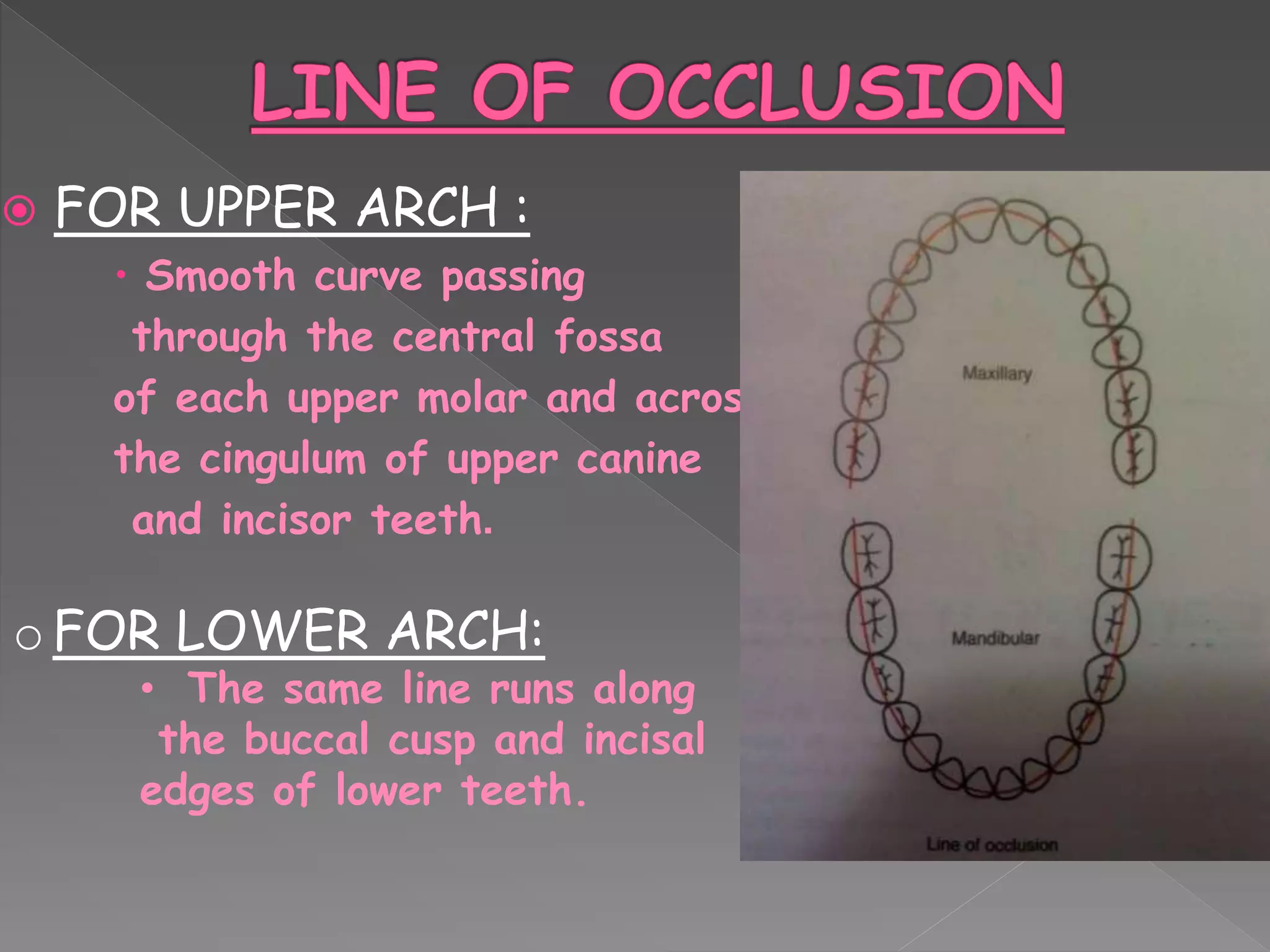

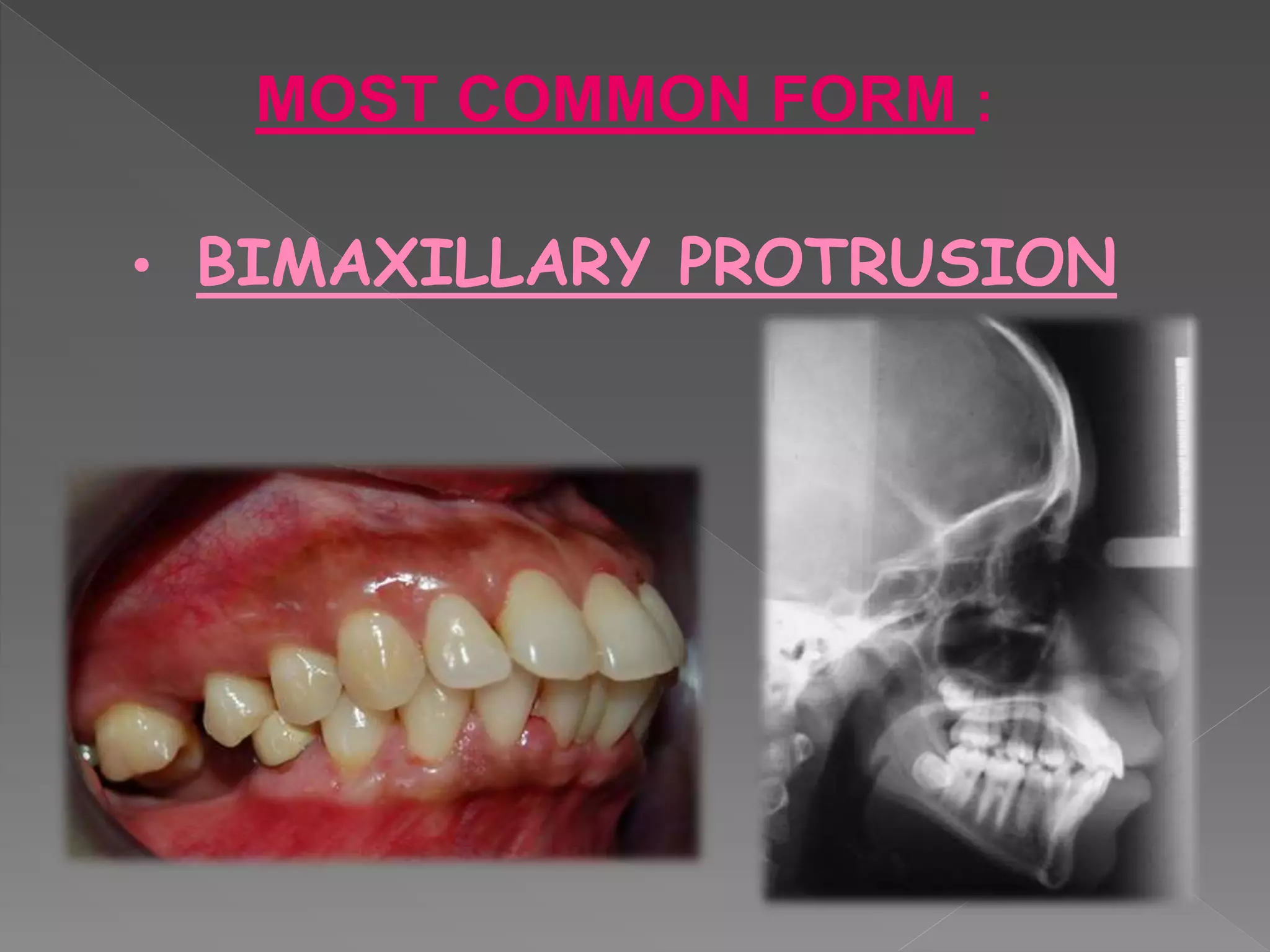
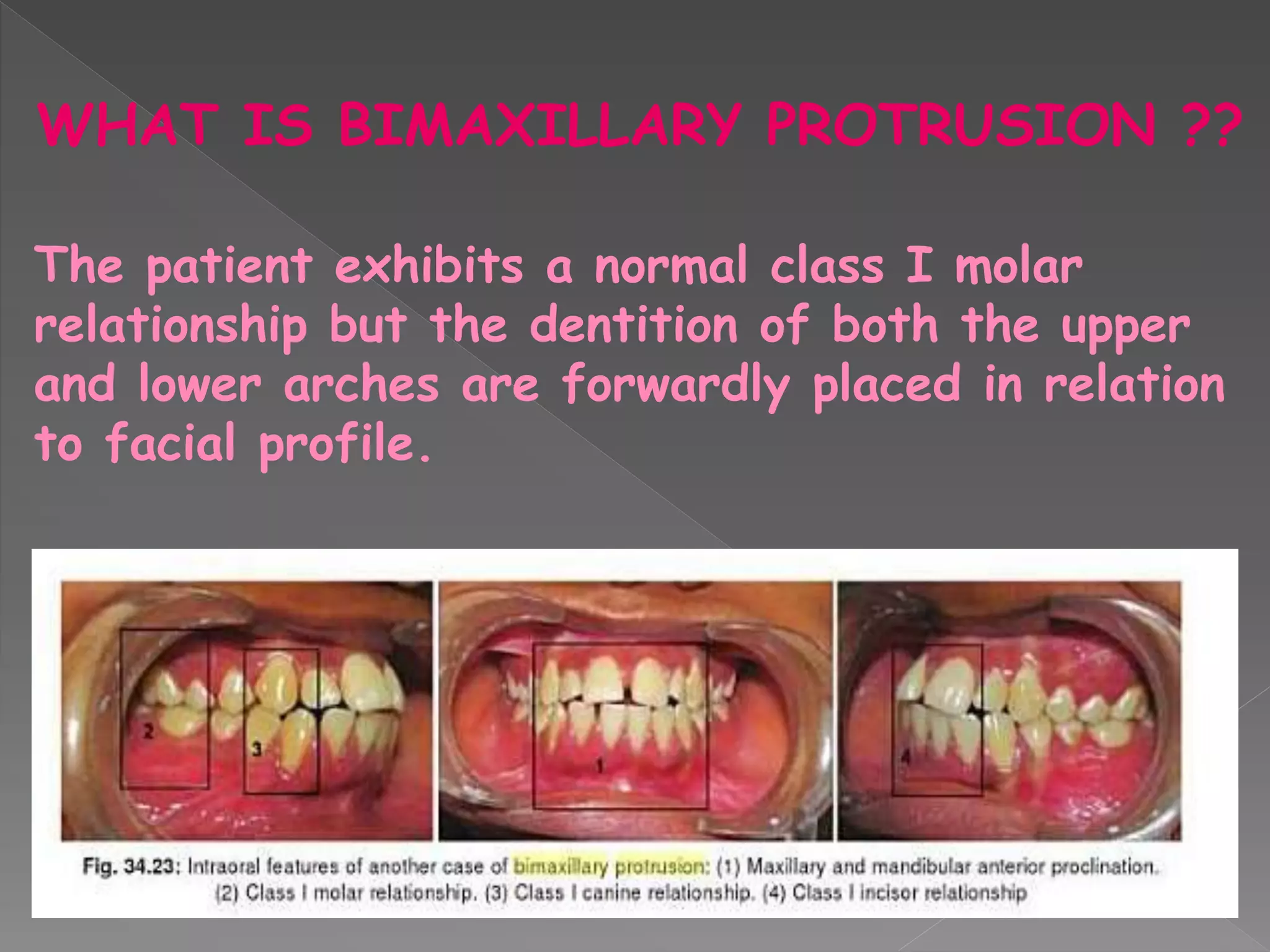
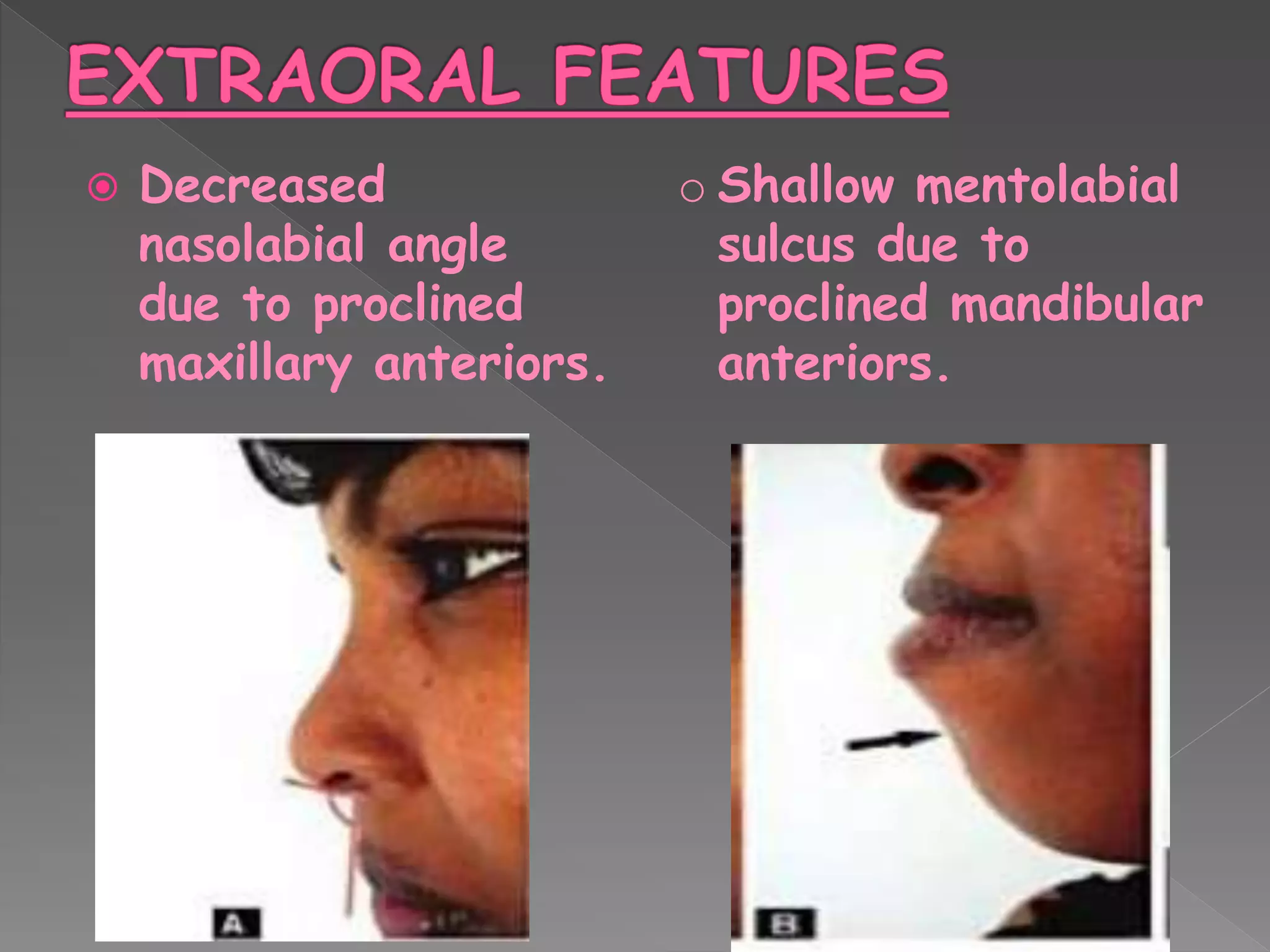
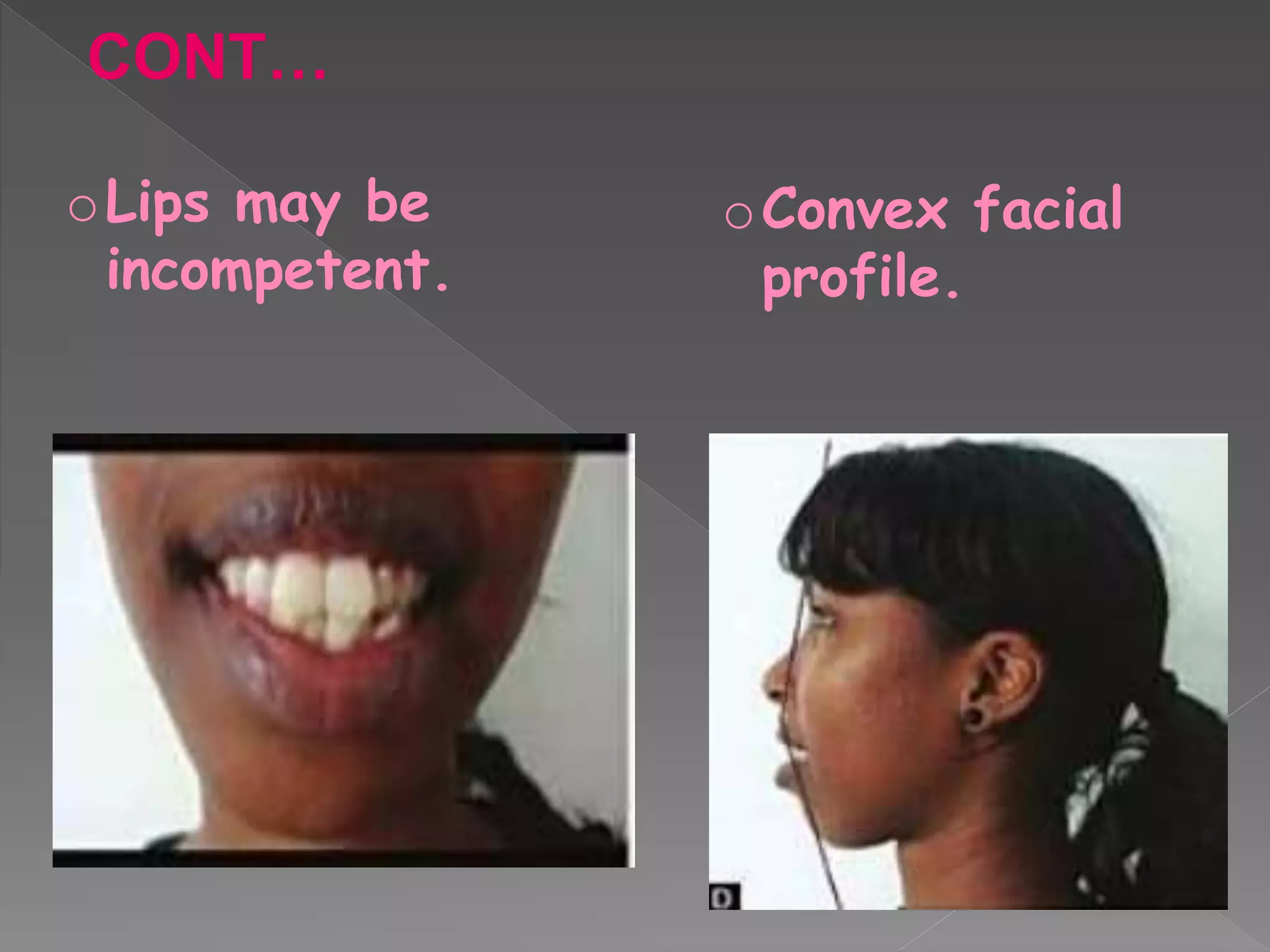
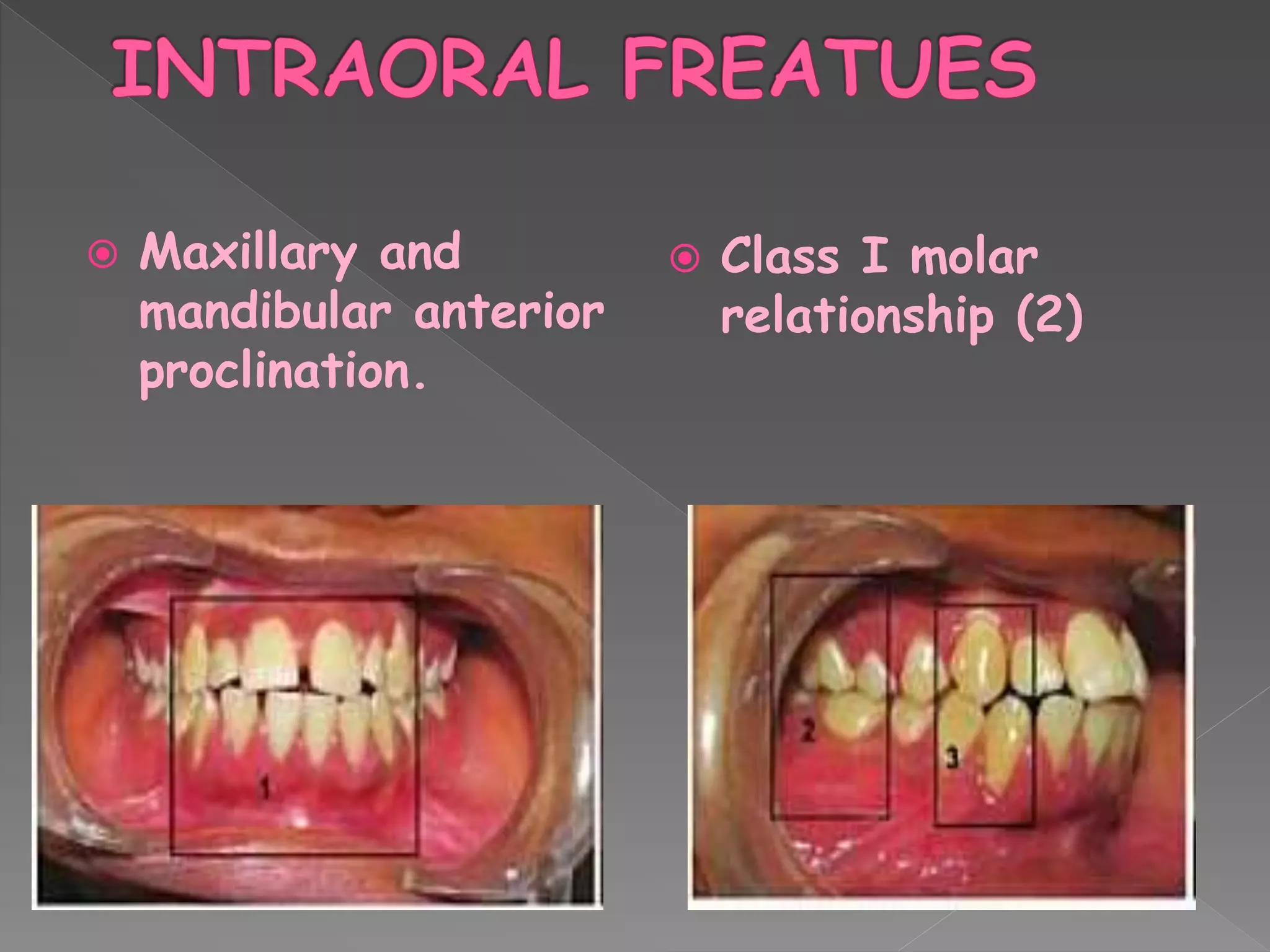

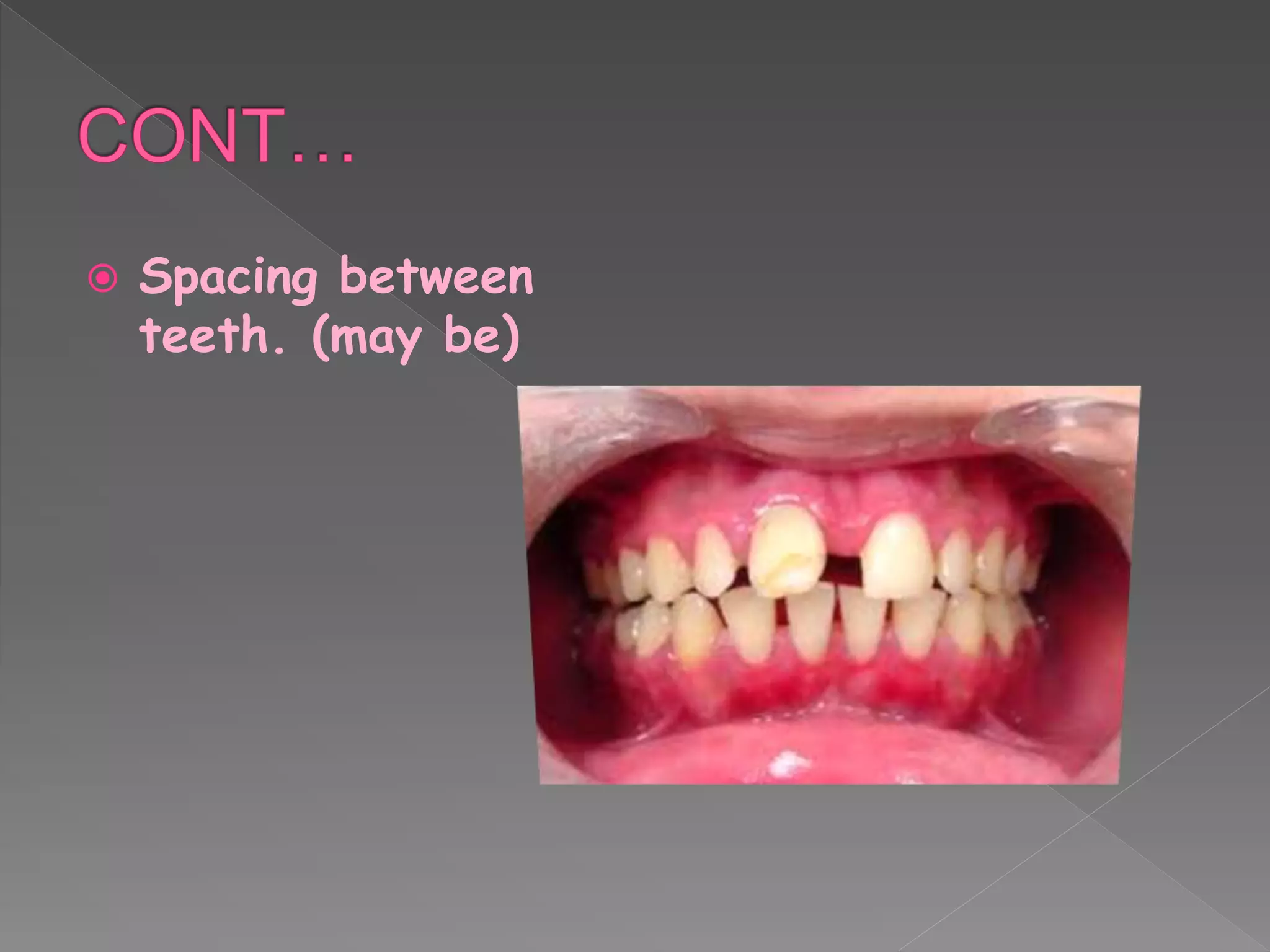
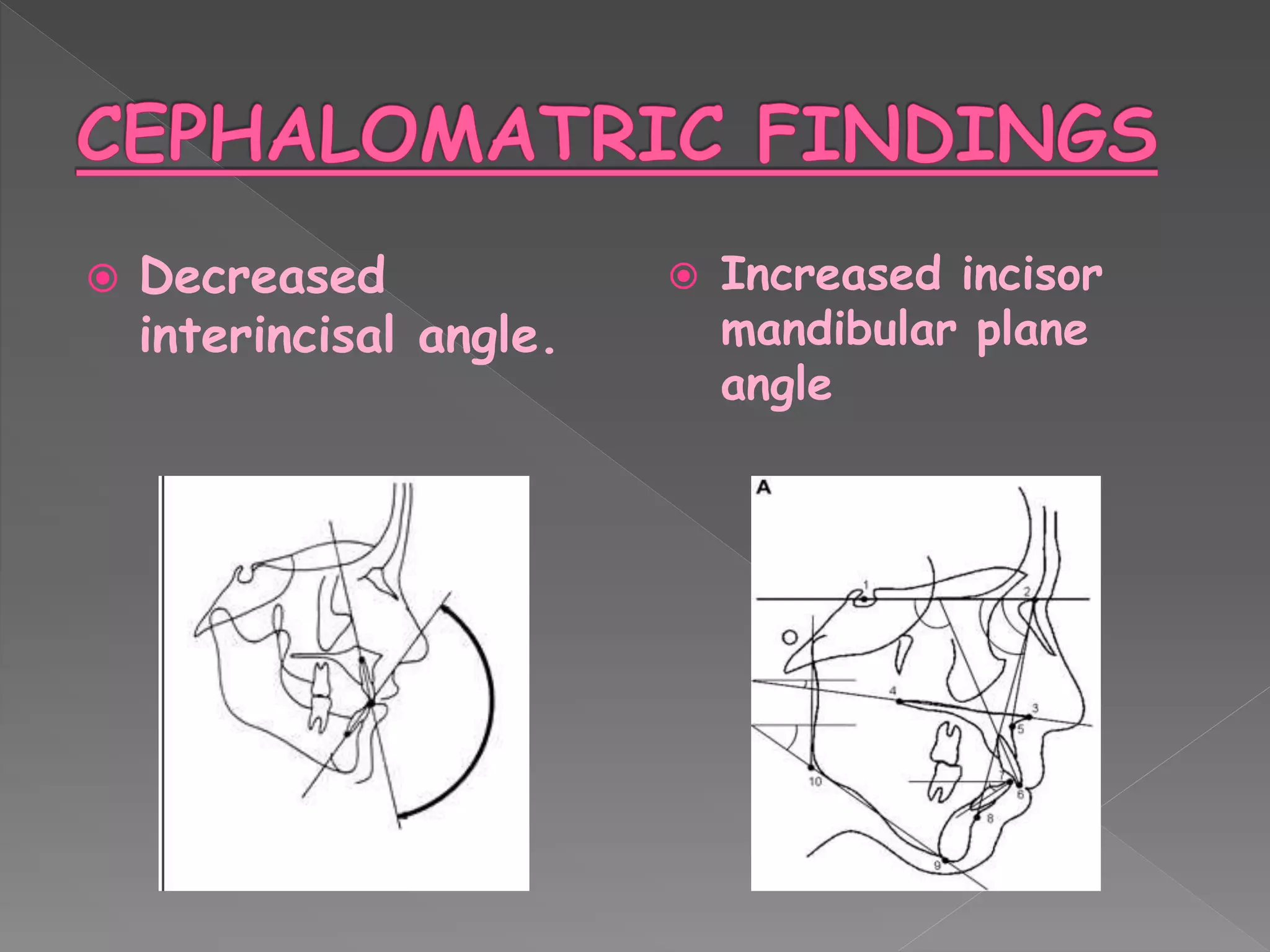
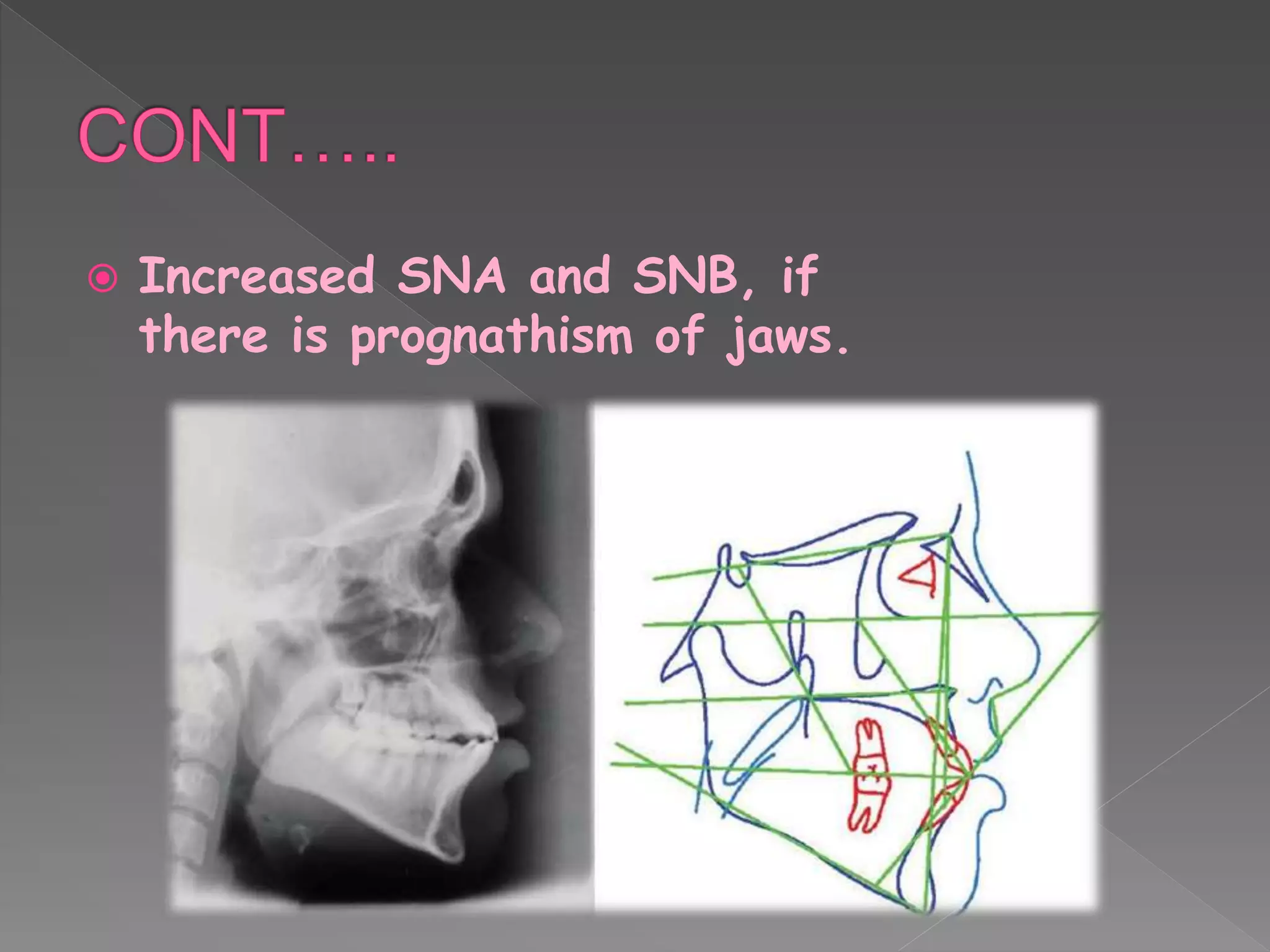

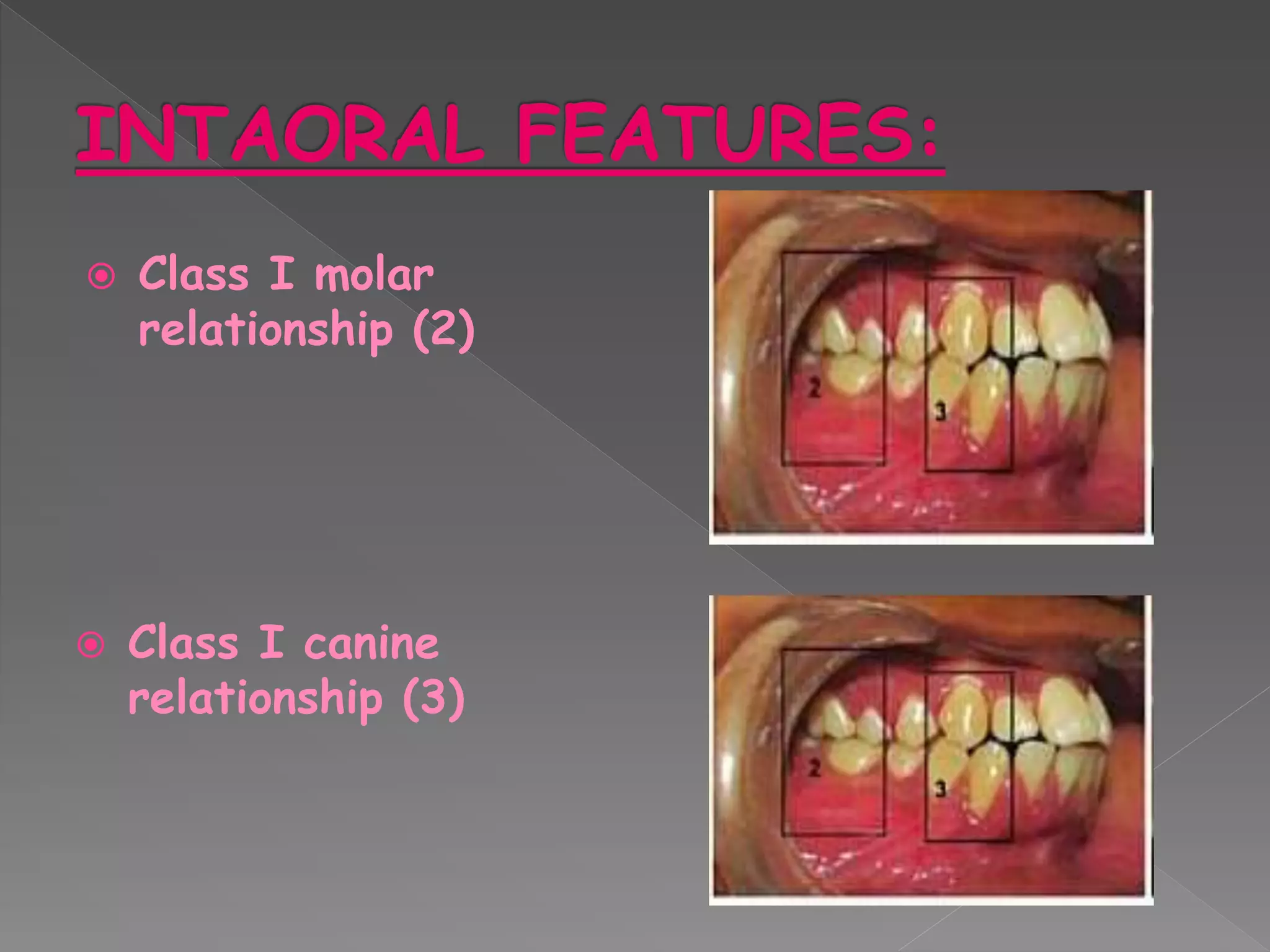

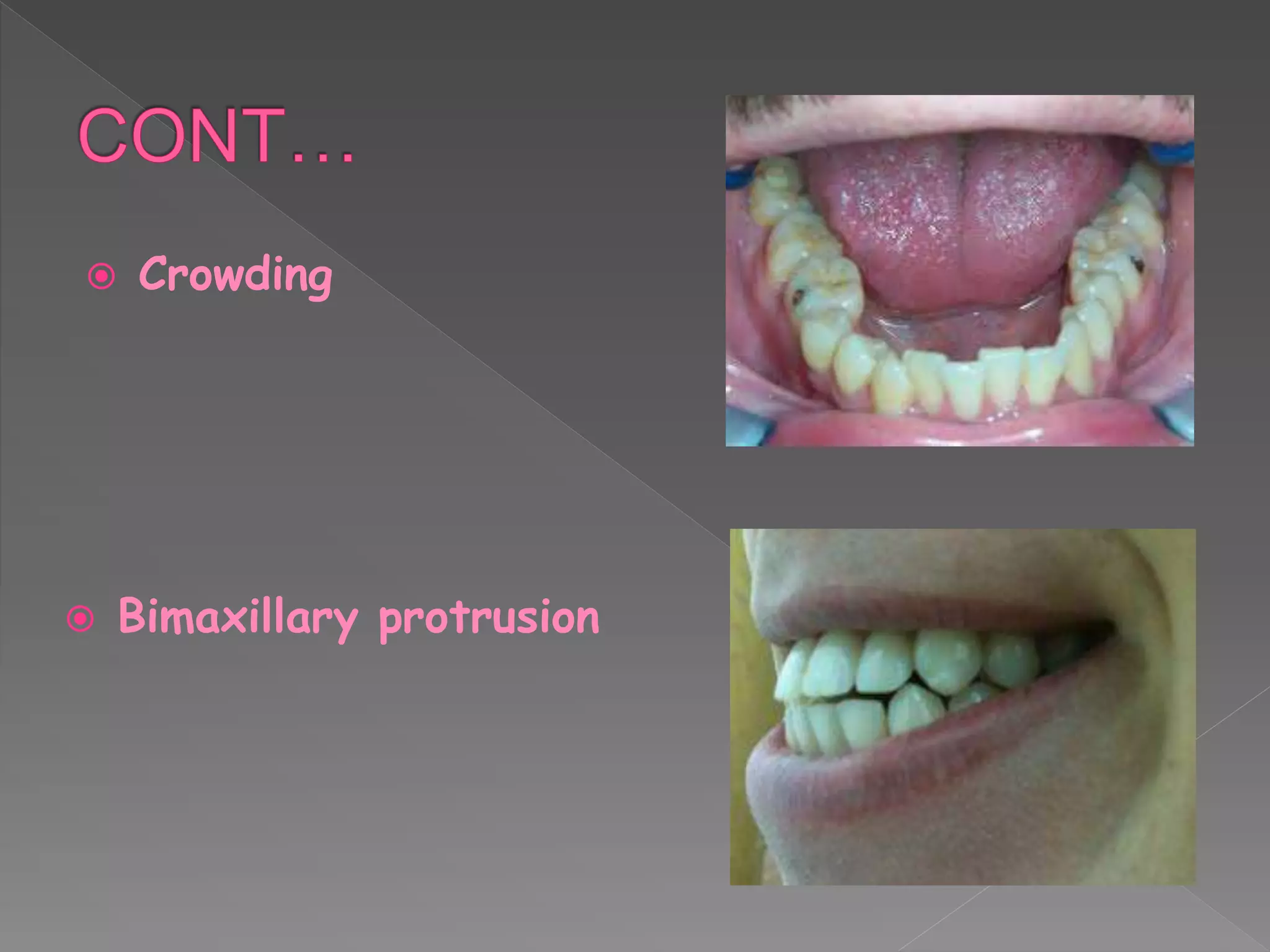














This document discusses class I malocclusion and its management. It defines occlusion and class I occlusion. Class I malocclusion occurs when the molar relationship is class I but the line of occlusion is incorrect. Common causes include genetic and developmental factors. Bimaxillary protrusion is the most common type, characterized by maxillary and mandibular anterior proclination. Management depends on the specific malocclusion, and may include appliances, extractions, and in severe cases, orthognathic surgery.


















































![Classification_of_malocclusion[1] [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/classificationofmalocclusion1read-only-240212164016-9b5c21cb-thumbnail.jpg?width=640&height=640&fit=bounds)




































