

















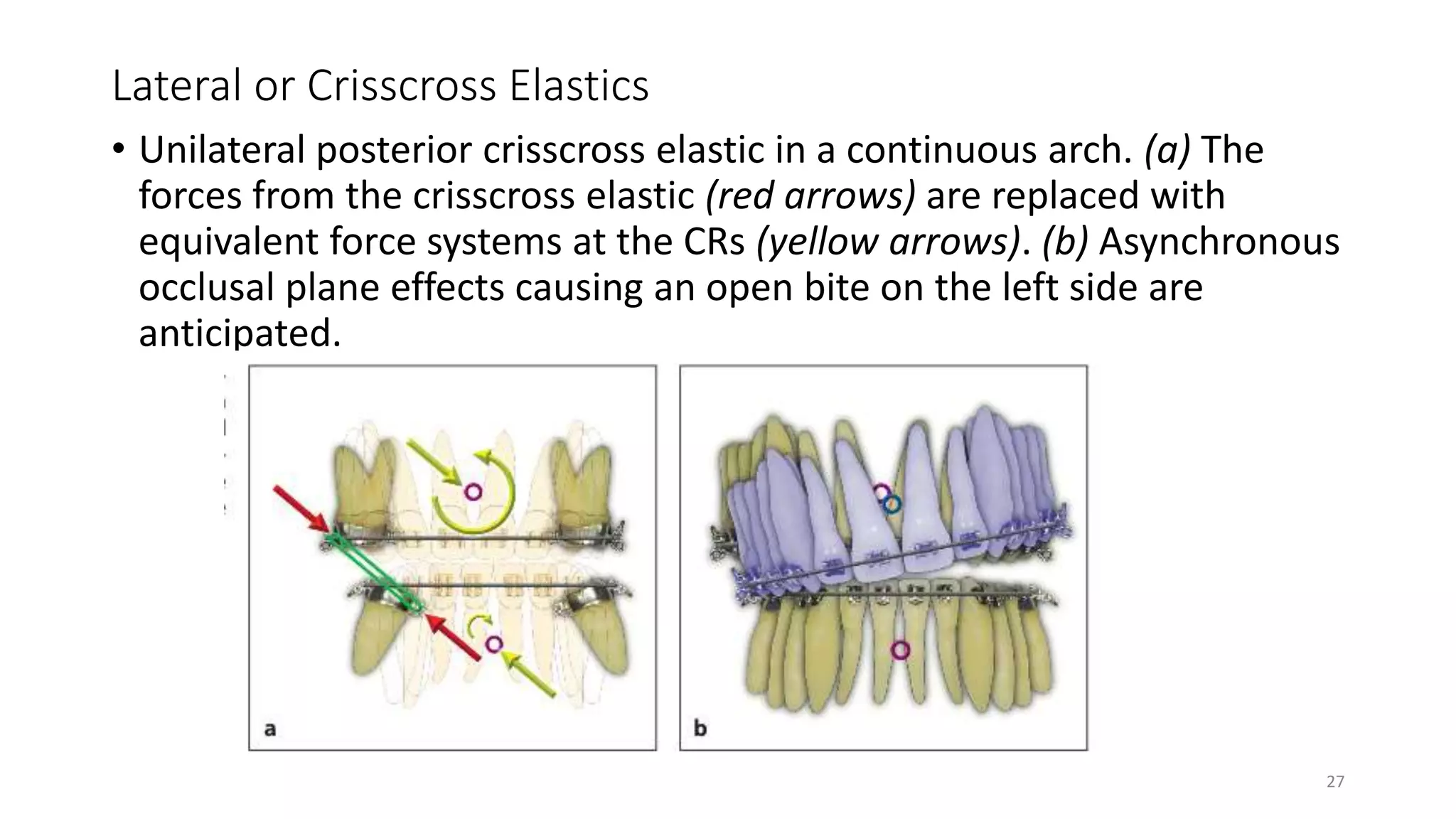

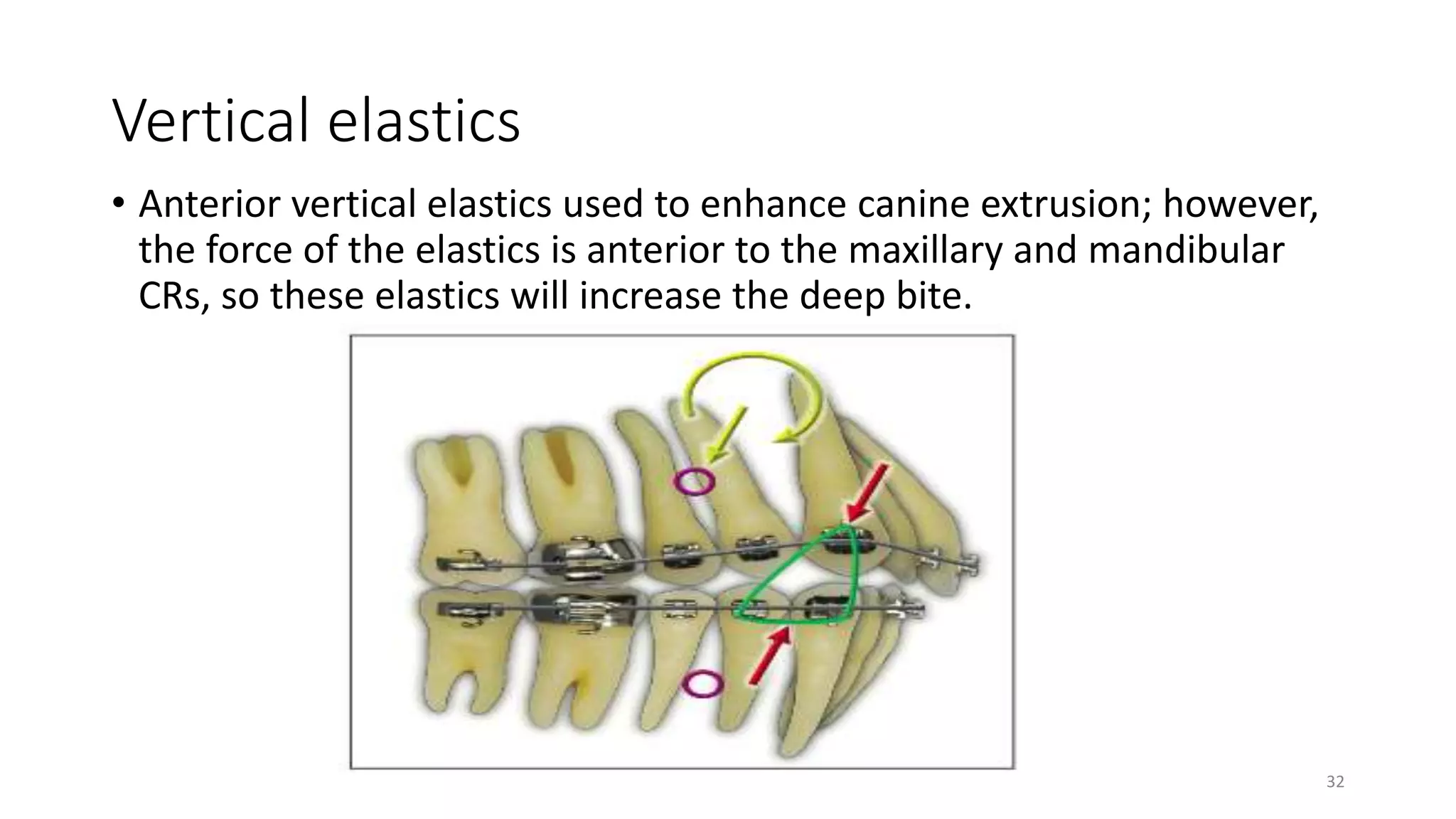
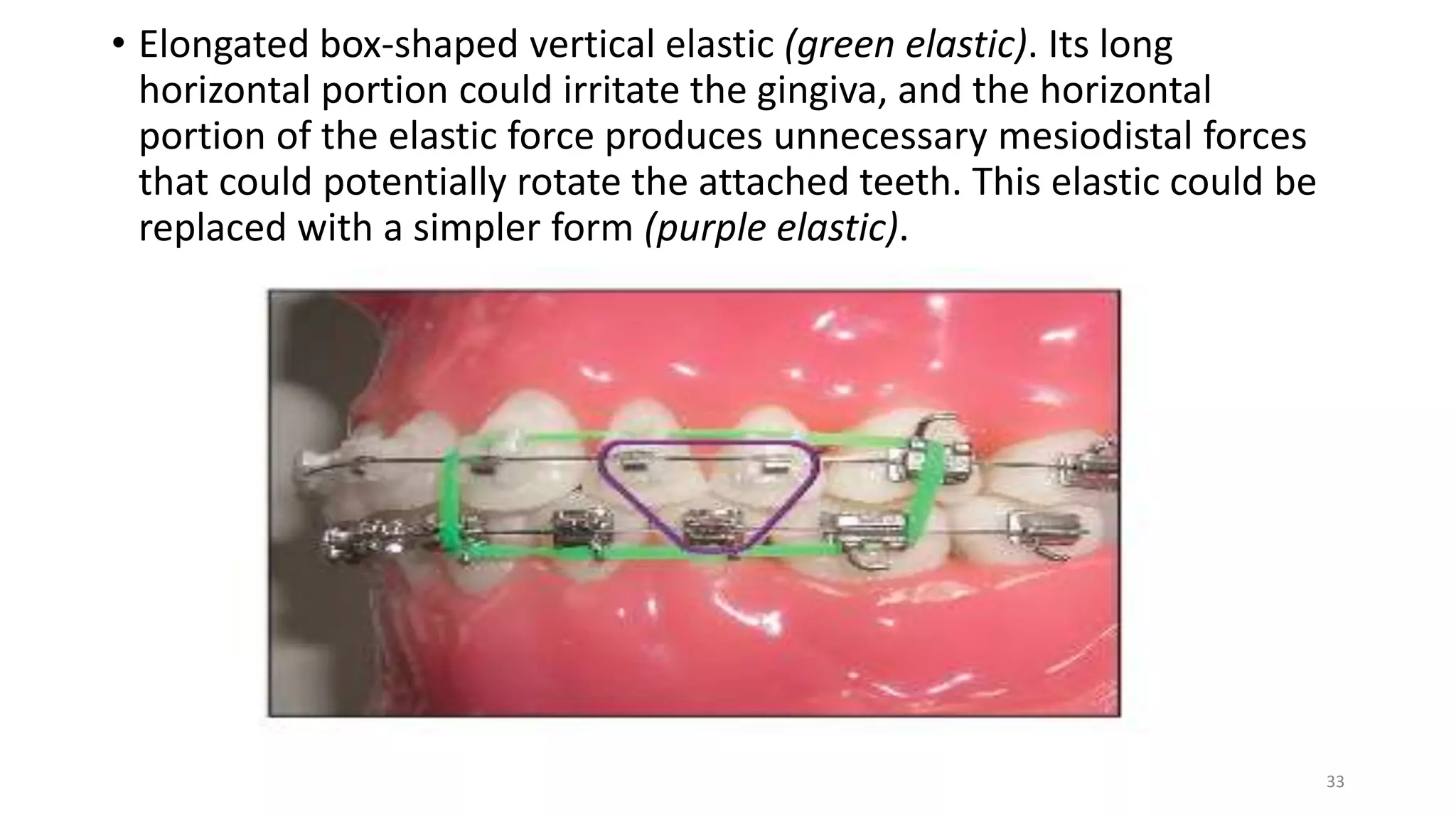








Elastics in orthodontics are essential tools used to correct malocclusions by applying forces to teeth, categorized based on their movement direction, size, and application mechanics. The document details the complexities of different elastics, their force levels, and the biomechanical principles governing their use, emphasizing the need for proper understanding to avoid complications. It concludes that elastics are indispensable in orthodontic treatment and that their appropriate application can significantly benefit patient outcomes.









































![Alexander_Discipline_(PART_2)[1] complete.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/alexanderdisciplinepart21-251118184023-04d0c3b3-thumbnail.jpg?width=640&height=640&fit=bounds)

































