Downloaded 251 times




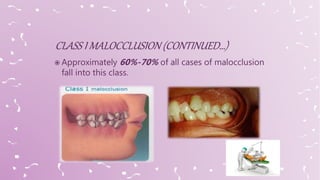

















The document discusses Class I malocclusion, including its characteristics, causes, features, and various treatment options depending on the specific dental irregularities present such as spacing, crowding, crossbites, open bites, and deep bites. Common treatment approaches involve the use of removable or fixed appliances to align teeth and resolve the malocclusion. Retention is emphasized as important to maintain stability after active treatment.























































































