Downloaded 262 times






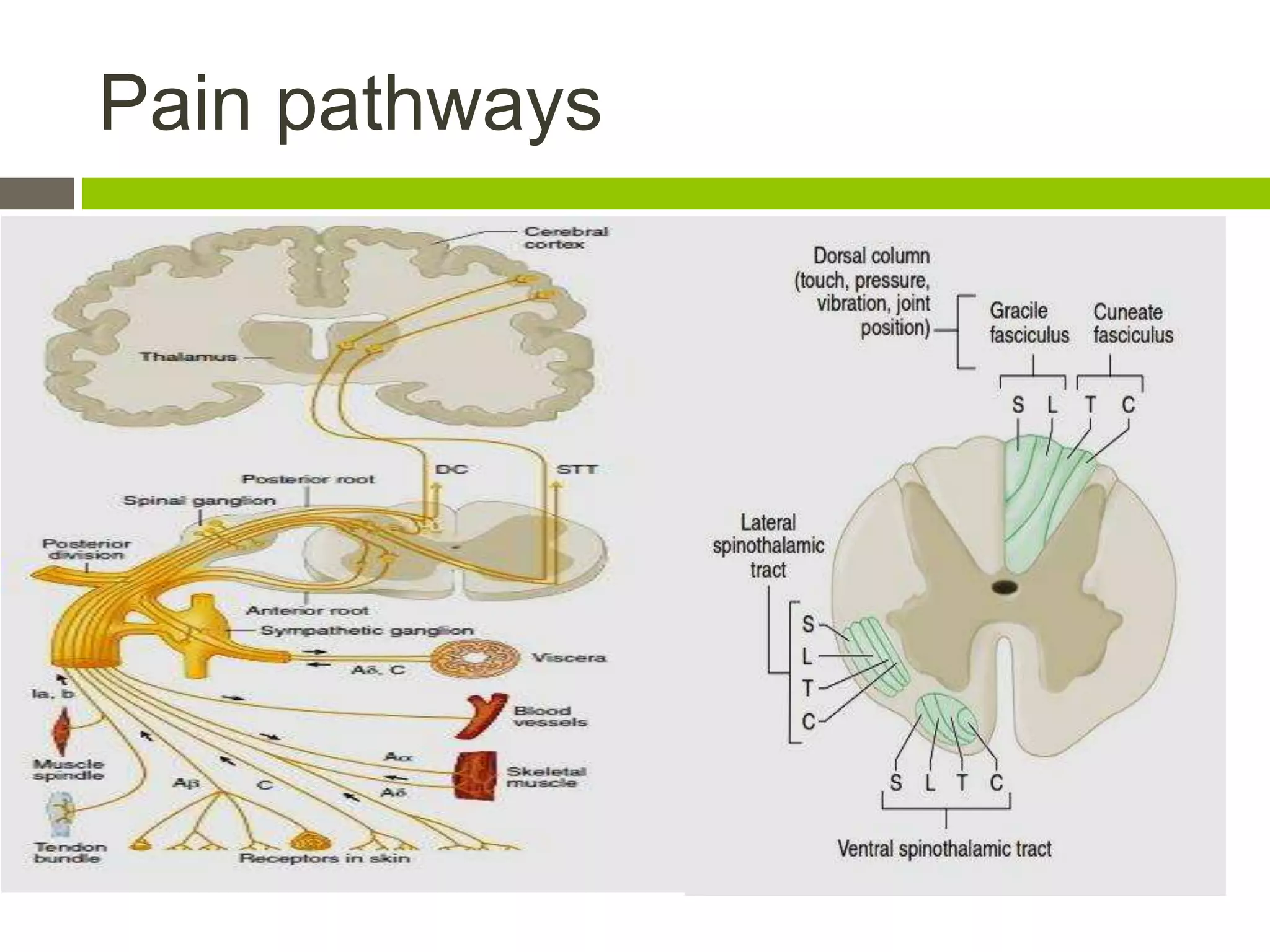










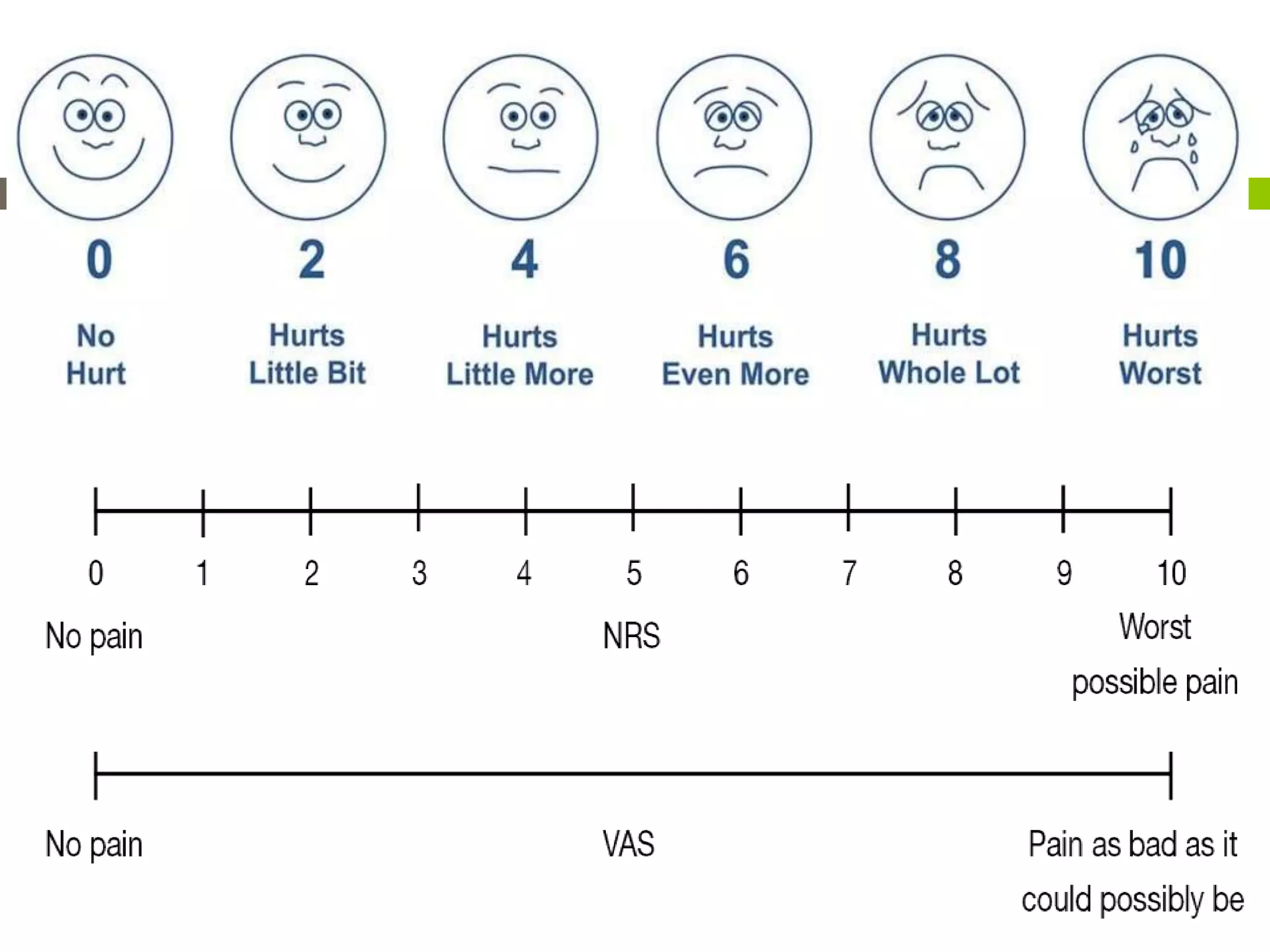





























This document discusses chronic pain management. It defines chronic pain as pain that lasts months or years in any part of the body and can lead to depression, anxiety, and sleep issues. Chronic pain differs from acute pain in that it continues long after an injury heals. The document describes three types of chronic pain - neuropathic, somatic, and visceral - and their characteristics. It discusses evaluating and measuring pain, as well as pharmacological, physical, psychological, and invasive treatment methods for managing chronic pain. The goal of chronic pain treatment is to improve daily functioning and quality of life by decreasing pain and suffering through a multidisciplinary approach.























































































