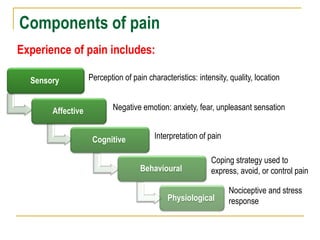
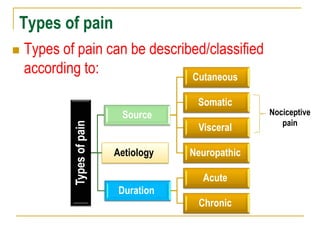
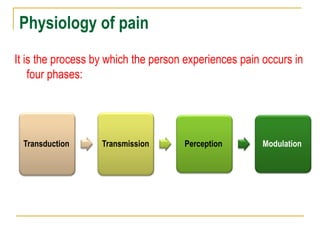
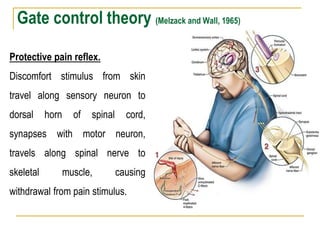
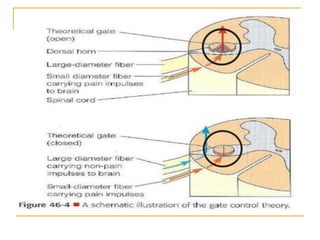
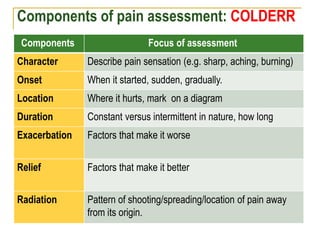
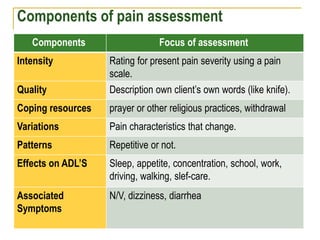
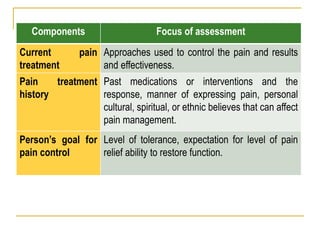
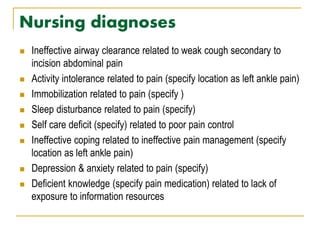
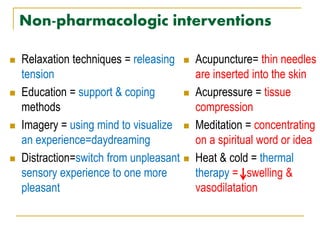
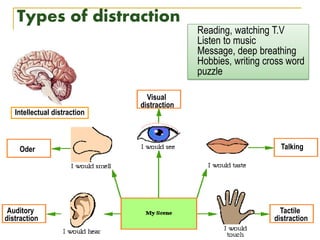
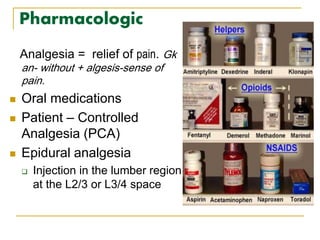
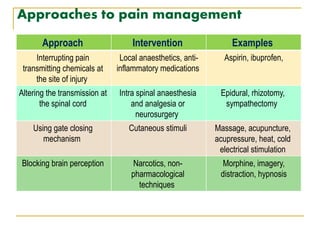
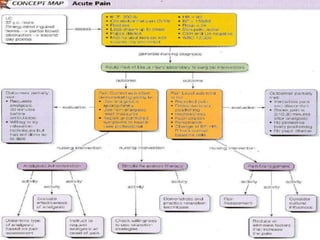

The document discusses pain management. It defines pain and describes its components and types. It outlines the physiology of pain through four phases: transduction, transmission, perception, and modulation. It also discusses nursing assessments of pain, common nursing diagnoses for patients in pain, and approaches to pain management, including pharmacological and non-pharmacological interventions as well as health teaching.