
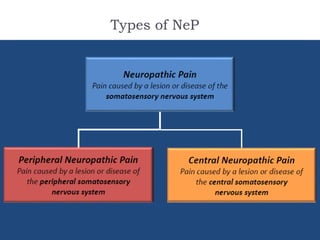
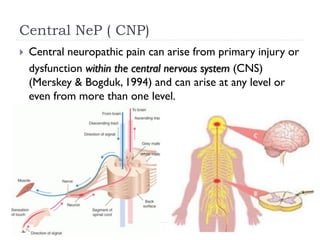


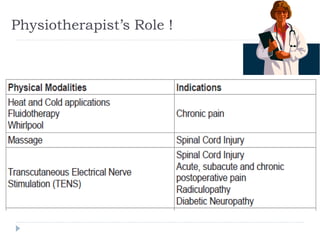


- Neuropathic pain is caused by damage or disease affecting the somatosensory nervous system and is difficult to diagnose due to its subjective nature. It can be central (originating from the central nervous system) or peripheral (originating from the peripheral nervous system) in nature. - Pathophysiological mechanisms involve hyperactivity of nociceptors leading to secondary changes in neurons processing somatosensory information. Diagnosis involves detailed history, neurological exam, and assessment tools to identify neuropathic features. - Treatment includes pharmacological interventions like antidepressants, anticonvulsants, opioids, and topical agents as well as physical therapy modalities like exercise, stretching, strengthening, hydrotherapy, graded motor imagery,














































































