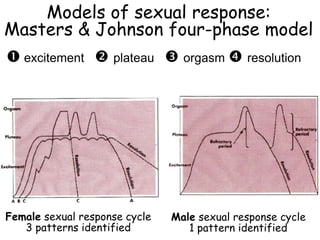
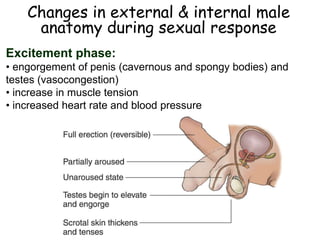
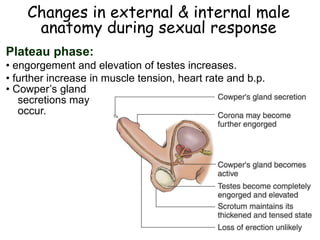
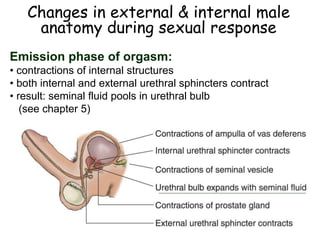
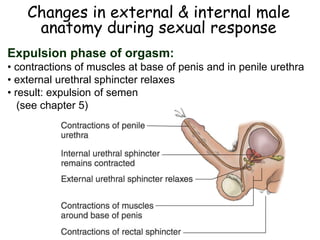
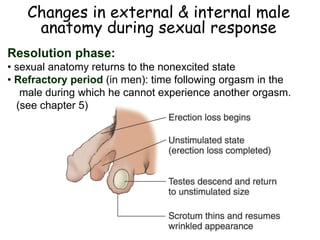
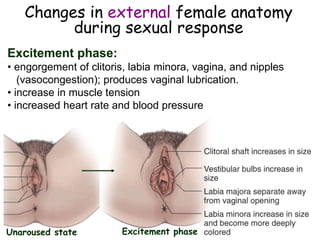
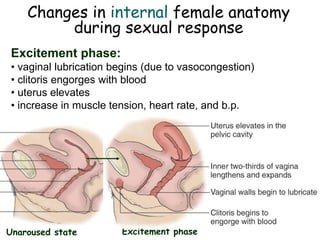
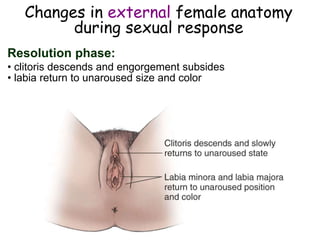
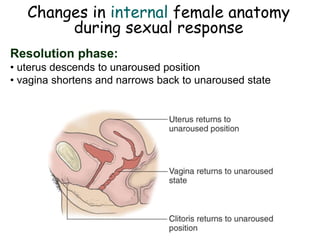
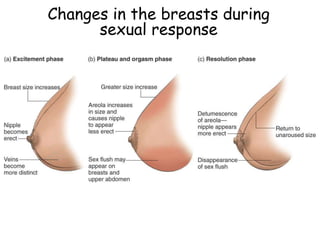
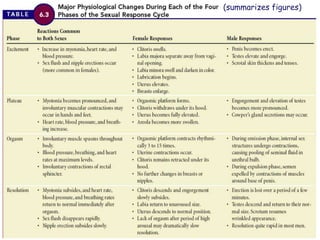
This document summarizes key points about hormones and the brain in relation to sexual arousal and response. It discusses how testosterone and estrogen influence male and female libido. The limbic system and neurotransmitters like dopamine and oxytocin facilitate sexual arousal. Visual, tactile, and olfactory senses can stimulate arousal depending on cultural conditioning. The document also describes Masters and Johnson's four phase model of sexual response and changes in male and female anatomy that occur during each phase. It addresses historical misconceptions about female sexuality and explores the purported "G-spot".


















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)





![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)









