Downloaded 57 times
![CHOLINERGIC DRUGS
[PARASYMPATHOMIMETICS]
DR. RAMESH KRISHNAN
MD,PHARMACOLOGY[2 ND YEAR]](https://image.slidesharecdn.com/cholinergicramesh-170719142000/85/Cholinergic-ramesh-1-320.jpg)
![CHOLINERGIC DRUGS
[PARASYMPATHOMIMETICS]
DR. RAMESH KRISHNAN
MD,PHARMACOLOGY[2 ND YEAR]](https://image.slidesharecdn.com/cholinergicramesh-170719142000/75/Cholinergic-ramesh-1-2048.jpg)
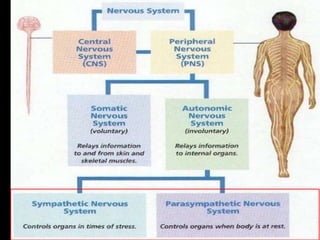
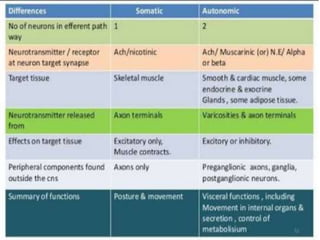
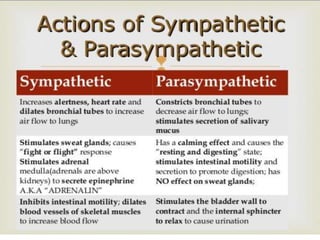
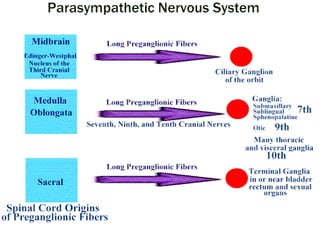
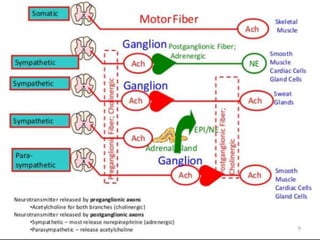
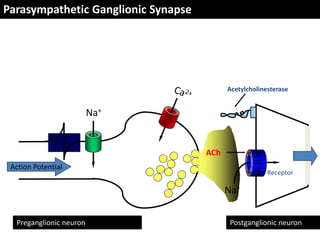


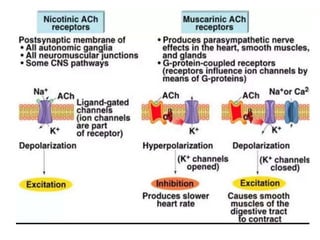
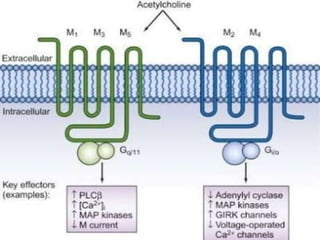
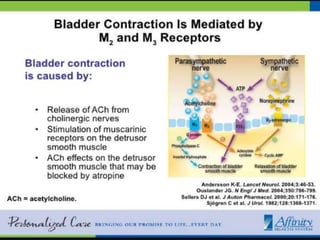
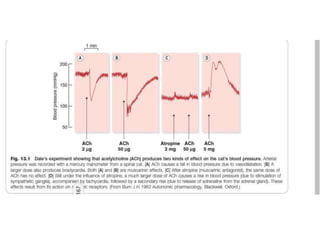
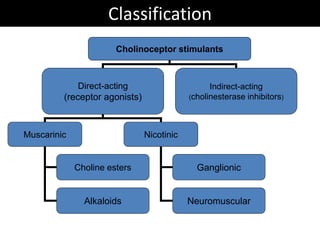
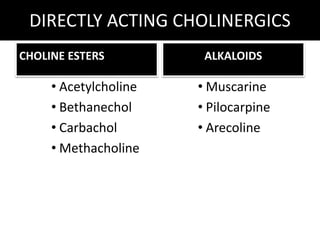
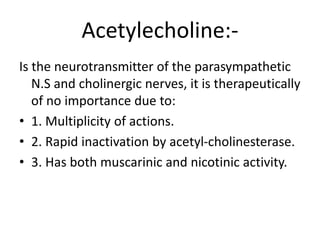
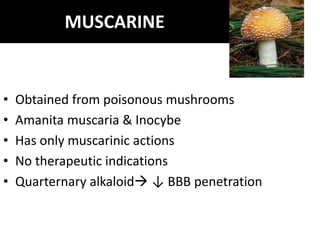
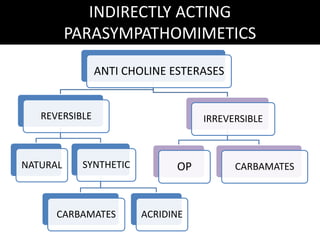
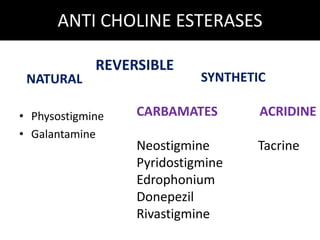
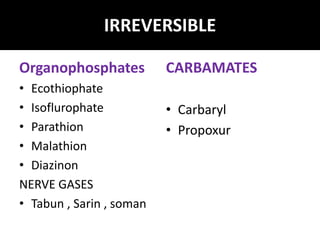
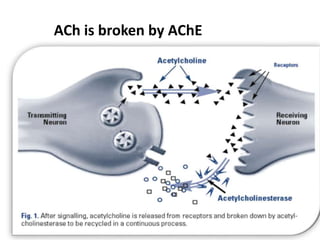
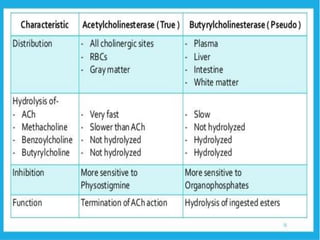
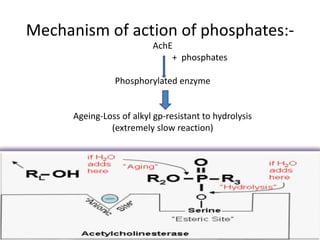
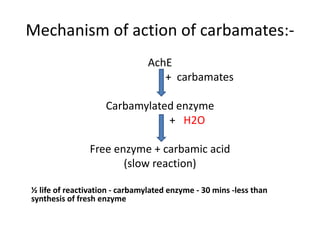
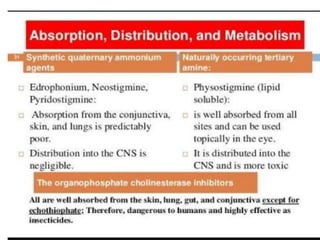
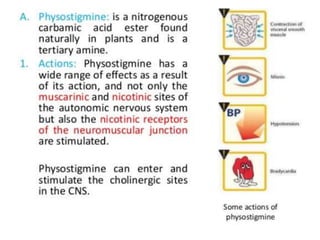
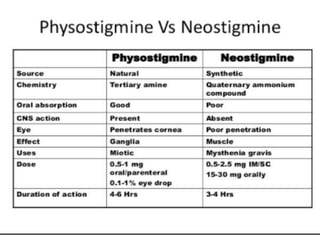
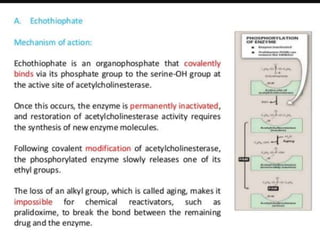
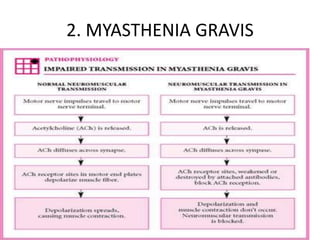
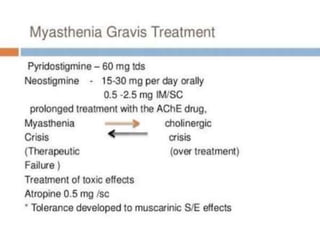
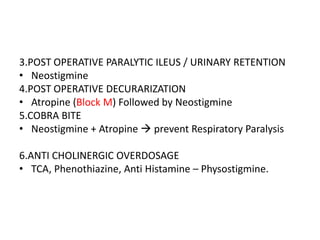
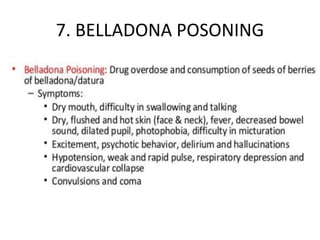
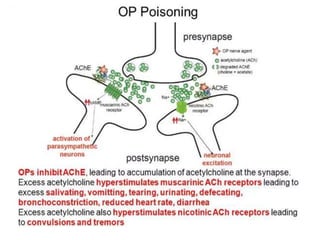


This document discusses cholinergic drugs, which act on the parasympathetic nervous system. It describes two main types: direct-acting cholinergics (acetylcholine and related agonists) and indirect-acting cholinergics (cholinesterase inhibitors). The direct-acting drugs include acetylcholine, pilocarpine, and muscarine. The indirect-acting drugs inhibit the enzyme acetylcholinesterase, increasing cholinergic activity. Examples given are physostigmine, neostigmine, pyridostigmine, and organophosphate nerve agents. The document outlines the mechanisms and uses of these drugs in conditions like glaucoma, myasthenia gravis,























































































