•Learning Objectives
•Define cholinergicand anticholinergic drugs and classify them
based on mechanism of action.
•Describe acetylcholine synthesis, release, receptors (muscarinic
& nicotinic), and termination of action.
•Explain the pharmacological actions, therapeutic uses, adverse
effects, and contraindications of cholinergic drugs.
•Explain the pharmacological actions, therapeutic uses, adverse
effects, and contraindications of anticholinergic drugs.
•Differentiate between cholinergic crisis and anticholinergic
toxicity based on clinical features and management.
•Apply knowledge to clinical scenarios, including organophosphate
poisoning and atropine use.
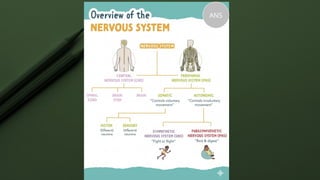
Parasympathetic Nervous System
•Works to save energy, aids in digestion, and
supports restorative, resting body functions-
Rest & Digest.
–Decrease in heart rate
–Increased gastro intestinal tract tone and
peristalsis
–Urinary sphincter relaxation
–Vasodilation – decrease in blood pressure
6.
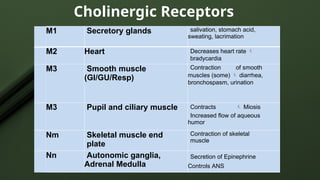
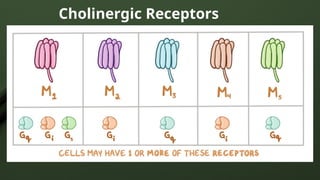
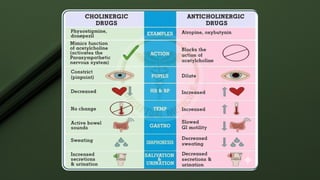
Cholinergic Receptors
M1 Secretoryglands salivation, stomach acid,
sweating, lacrimation
M2 Heart Decreases heart rate
bradycardia
M3 Smooth muscle
(GI/GU/Resp)
Contraction of smooth
muscles (some) diarrhea,
bronchospasm, urination
M3 Pupil and ciliary muscle Contracts Miosis
Increased flow of aqueous
humor
Nm Skeletal muscle end
plate
Contraction of skeletal
muscle
Nn Autonomic ganglia,
Adrenal Medulla
Secretion of Epinephrine
Controls ANS
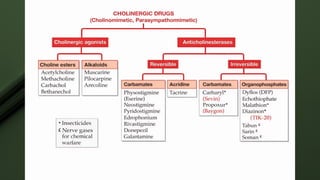
Cholinergic Drugs
• Oftencalled parasympathomimetic drugs, because their
action mimics the action of the PSNS.
• Also called as cholinomimetic.
• Stimulate parasympathetic nervous system in same manner
as acetylcholine
• Cholinergic agonists are two types :
• 1.Direct acting
2.Indirect acting
11.
Direct acting cholinergicagonist
• They act by binding directly to cholinoceptors.
• Direct acting cholinergics are lipid insoluble.
• Do not readily enter the CNS so effects are peripheral.
• Resistant to metabolism by acetylcholinesterase.
• Effects are longer acting than with acetylcholine.
• Acetylcholine
• Methacholine Muscarine
• Carbachol Pilocarpine
• Bethanechol Arecoline
12.
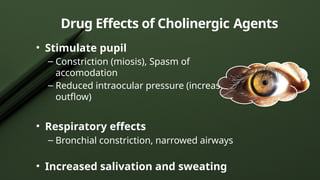
Drug Effects ofCholinergic Agents
• Cardiovascular effects
– Decreased HR( Bradycardia)
– Vasodilation (NO mediated)
• Stimulate intestine and bladder
– Increased gastric secretions
– Increased gastrointestinal motility
– Increased urinary frequency
Drug Effects ofCholinergic Agents
“MSLUBDD”
Many Smart Ladies Ultimately Bring Disaster for Dudes!
• Miosis
• Salivation
• Lacrimation
• Urination
• Bronchoconstriction
• Defaecation
• Decreased heart rate
15.
Acetylcholine
• One ofthe main neurotransmitters of the ANS is
acetylcholine
• Acetylcholine is released at preganglionic fibers of
both the sympathetic and parasympathetic nervous
system
• Also released from postganglionic sympathetic
neurons that innervate the sweat glands and from
motor neurons that innervate the skeletal muscles
17.
Acetylcholine
• It isa quaternary ammonium compound so cannot
penetrate the membrane.
• Does not have any therapeutic importance, because
rapid inactivation by acetylcholinesterases.
• It has both Muscarinic & Nicotinic actions .
18.
Bethanechol
• Not hydrolyzedby acetylcholinesterases.
• Actions:
• Directly stimulates M receptors causing increased
intestinal motility & tone.
• It stimulates detrusor muscle of the bladder while
trigone & sphincters are relaxed causing expulsion of
urine.
Pilocarpine
An alkaloid, lipidsoluble & is stable to hydrolysis by
cholinsterases.
Actions:
When applied locally to cornea produces rapid miosis
& contraction of ciliary muscle produces spasm of
accommodation.
Therapeutic Use :
In Glaucoma it opens trabecular meshwork around
schlemm’s canal
• causes drainage of aqueous humor
• IOP immediately decreases.
21.
Indirect acting Cholinergicagonists
• They act through inhibition of Acetyl cholinesterase
enzyme, so increase Acetylcholine level in the synapse.
• Accumulation of acetylcholine then occurs which
enhances the activation of the nicotinic and
muscarinic receptors.
• Anticholinesterase drugs are either reversible or
irreversible inhibitors of acetylcholinesterase.
• Physostigmine -
-onlyanticholinesterase capable of crossing the
blood brain barrier.
-Is more lipid soluble.
-Used as an antidote for overdosage of
anticholinergics such as: atropine,
antihistamines, TCA, phenothiazines.
-May also be used in treatment of glaucoma.
24.
• Pyridostigmine -
•is the maintenance drug of choice for
patients with Myasthenia gravis.
• Neostigmine –
• prototype anticholinesterase agent.
• Used for long-term treatment of
myasthenia gravis and as an antidote for
tubocurarine and other non- depolarizing
agents in surgery.
25.
• Donepezil -
•Used in the treatment of mild to
moderate Alzheimer’s disease.
• Helps to increase or maintain memory and
learning capabilities.
26.
Uses of IndirectCholinergic agonists
• Glaucoma – Pilocarpine, Physostigmine
• Edrophonium to test Myasthenia gravis,
Neostigmine and pyridostigmine in treatment of
M.gravis.
• Postoperative paralytic ileus - Neostigmine
• Postoperative decurarization –
Neostigmine(reverses muscle paralysis)
Cholinergic Agents: SideEffects
Side effects are a result of overstimulation of the
PSNS.
• Cardiovascular:
– Bradycardia, hypotension, conduction
abnormalities (AV block and cardiac arrest)
• CNS:
– Headache, dizziness, convulsions
• Gastrointestinal:
– Abdominal cramps, increased secretions, nausea,
vomiting
29.
Cholinergic Agents: SideEffects
• Respiratory:
–Increased bronchial secretions,
bronchospasms
• Other:
–Lacrimation, sweating, salivation, loss of
binocular accommodation, miosis
30.
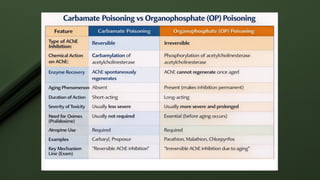
Acute toxic effectsof irreversible
cholinesterase inhibitors (OP poisoning )
• These agents are lipid soluble
• Can enter the body by the eye,skin, respiratory
system and GI tract.
• organophosphate insecticides (malathion, parathion)
or nerve gases (sarin, tabun, soman)
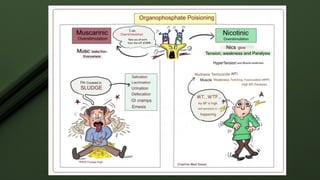
• These agents cause excessive cholinergic
stimulation (muscarinic) and neuromuscular
blockade
33.
Treatment of OPpoisoning
Emergency treatment includes:
• Decontamination of clothing
• Flushing poison from skin and eyes
• Activated charcoal and lavage for GI ingestion
• Atropine to counteract the muscarinic effects
(2mg IV every 10 min till pupil dilates, max 50-
100mg)
34.
• To relievethe neuromuscular blockade by
nicotinic effects, give pralidoxime, a
cholinesterase reactivator.
• Pralidoxime causes the anticholinesterase
poison to release the enzyme
acetylcholinesterase.
• Give Pralidoxime as soon as possible as if too
much time passes, the poison bond becomes too
strong (aging) for the pralidoxime to work.
36.
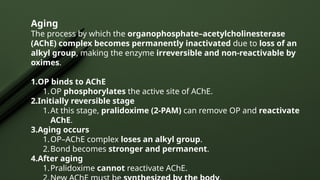
Aging
The process bywhich the organophosphate–acetylcholinesterase
(AChE) complex becomes permanently inactivated due to loss of an
alkyl group, making the enzyme irreversible and non-reactivable by
oximes.
1.OP binds to AChE
1.OP phosphorylates the active site of AChE.
2.Initially reversible stage
1.At this stage, pralidoxime (2-PAM) can remove OP and reactivate
AChE.
3.Aging occurs
1.OP–AChE complex loses an alkyl group.
2.Bond becomes stronger and permanent.
4.After aging
1.Pralidoxime cannot reactivate AChE.
37.
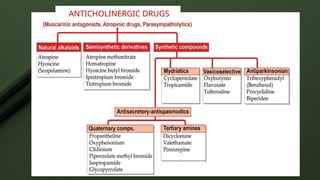
• Drugs thatblock or inhibit the actions of
acetylcholine (ACh) in the parasympathetic
nervous system (PSNS).
• Also called cholinergic blocking agents or
parasympatholytics.
• Often referred to as anticholinergics or
antimuscarinics
What are anticholinergics
38.
Mechanism of Action
•Competitive antagonists
• Compete with acetylcholine
• Reversible blockade of acetylcholine at
muscarinic receptors by competitive binding
• Once these drugs bind to receptors, they inhibit
nerve transmission at these receptors.
Actions
Cardiovascular effects-
• Decreasedcardiovascular response to vagal
stimulation resulting in tachycardia
• Tachycardia due to antagonism of the vagal affect.
• Vascular
– no (direct) effect
– except, dilate cutaneous vessels (red as a beet)
– block hypotensive effect of muscarinic agonists
43.
Actions
CNS –
• Atnormal doses atropine stimulates
medullary centers, However, at higher
doses produce excitement, agitation,
hallucinations and coma.
• Depresses vestibular excitation and has
anti motion sickness properties
• Supresses tremor and rigidity of
parkinsonism by blocking cholinergic
overactivity in basal ganglia.
44.
Actions
Eye:
• Dilated pupils(mydriasis)
• Blocks muscarinic innervations on the
circular muscles (Mydriasis) and relaxes
cilairy muscles (Cycloplegia)
• Worsens glaucoma
45.
Actions
Gastrointestinal:
• Relax smoothmuscles of GI tract
• Decrease intestinal and gastric secretions
• Decrease motility and peristalsis
• antispasmodic effect
• Sphincter contraction
46.
Respiratory system -
•Decreases bronchial secretion (used as
preanesthetic Medication, COPD)
• Dilated bronchial airways (used for treatment of
Asthma)
Actions
47.
Genitourinary -
• Relaxesdetrusor muscle
• Increased constriction of internal sphincter
• Result: urinary retention
• Relaxation of smooth muscles of ureters.
• Therefore, they are contraindicated for prostate
hypertrophy patients.
Actions
Therapeutic Uses
• AntidoteUses (Toxicology)
Atropine is a life-saving antidote for poisoning by
agents that excessively stimulate the cholinergic
system.
•Organophosphate Poisoning: This is a major
indication.
•Carbamate Insecticide Poisoning
•Certain Mushroom Poisoning: Effective against
mushrooms that contain muscarine (e.g., Amanita
muscaria).
51.
Treatment of OPpoisoning
Emergency treatment includes:
• Decontamination of clothing
• Flushing poison from skin and eyes
• Activated charcoal and lavage for GI ingestion
• Atropine to counteract the muscarinic effects (2mg IV
every 10 min till pupil dilates, max 50-100mg)
52.
• To relievethe neuromuscular blockade by
nicotinic effects, give pralidoxime, a
cholinesterase reactivator.
• Pralidoxime causes the anticholinesterase
poison to release the enzyme
acetylcholinesterase.
• Give Pralidoxime as soon as possible as if too
much time passes, the poison bond becomes too
strong (aging) for the pralidoxime to work.
53.
Therapeutic Uses
Central NervousSystem Disorders-
• Parkinson’s disease –
Benztropine,Trihexyphenidyl
• Those who cannot take Levodopa
• Helpful in decreasing salivation, spasticity and
tremors
• Motion Sickness (Scopolamine)
• Drug-induced extrapyramidal reactions(due to
antipsychotics)
54.
•CVS –
• Atropineis used to increase heart rate in
symptomatic bradycardias.
• Sinus node dysfunction
• Symptomatic second-degree heart block
• Sinus or nodal bradycardia (due to myocardial
infarction)
Therapeutic Uses
Toxicity of Anticholinergics
•Anticholinergic overdose
syndrome (Belladona
poisoning- consumption of
seeds or berries of belladona
or dhatura plant) is
characterized by:
- Hyperthermia, delirium, dry
mouth, tacycardia, ileus, urinary
retention. Seizures, coma and
respiratory arrest may occur.
66.
Toxicity of Anticholinergics
•Treatment –
- Gastric lavage with tannic acid, cold
sponging or ice bags, Physostigmine s.c.
or i.v., diazepam to control convulsions.
Individual Drugs
• Atropine- prototype. Antidote in OP Poisoning.
• Ipratropium - Useful in rhinorrhea. Also excellent
bronchodilator.
• Scopolamine - depresses CNS and causes amnesia,
drowsiness, euphoria, relaxation and sleep. Also good for
motion sickness. Given parenterally, orally and
transdermally.
• Benztropine - temporary use in Parkinson’s disease.
69.
Individual Drugs
• Trihexyphenidyl- also used for treating EPS by some
antipsychotics. Contraindicated in glaucoma.
• Flavoxate - relieves dysuria, urgency, frequency, and
pain with GU infections
• Oxybutynin - has direct antispasmodic effects on
smooth muscle and anticholinergic effects. Decreases
frequency of voiding.
70.
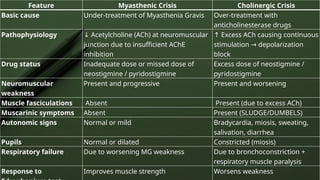
Feature Myasthenic CrisisCholinergic Crisis
Basic cause Under-treatment of Myasthenia Gravis Over-treatment with
anticholinesterase drugs
Pathophysiology ↓ Acetylcholine (ACh) at neuromuscular
junction due to insufficient AChE
inhibition
↑ Excess ACh causing continuous
stimulation depolarization
→
block
Drug status Inadequate dose or missed dose of
neostigmine / pyridostigmine
Excess dose of neostigmine /
pyridostigmine
Neuromuscular
weakness
Present and progressive Present and worsening
Muscle fasciculations Absent Present (due to excess ACh)
Muscarinic symptoms Absent Present (SLUDGE/DUMBELS)
Autonomic signs Normal or mild Bradycardia, miosis, sweating,
salivation, diarrhea
Pupils Normal or dilated Constricted (miosis)
Respiratory failure Due to worsening MG weakness Due to bronchoconstriction +
respiratory muscle paralysis
Response to Improves muscle strength Worsens weakness
Editor's Notes
#16 Botox is botulinum toxin type A. When injected into facial muscles, it blocks acetylcholine release at the neuromuscular junction by cleaving SNAP-25. Without acetylcholine, the muscle cannot contract, so it relaxes temporarily. As facial expressions reduce, the overlying skin smoothens and wrinkles disappear. The effect begins within a week and lasts for 3–6 months.”
#19 Paralytic ileus
Temporary paralysis of intestinal smooth muscle
Leads to absence of peristalsis
Causes abdominal distension, constipation, no bowel sounds
Common after surgery
Urinary retention
Inability to empty the urinary bladder completely
Due to failure of detrusor contraction or outlet obstruction
Results in bladder distension and discomfort
Post-surgical atony (bladder & GI tract)
Loss of smooth muscle tone after surgery
Occurs due to reduced parasympathetic activity
Leads to ileus in GI tract and urinary retention in bladder