Downloaded 36 times


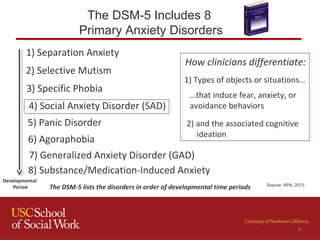
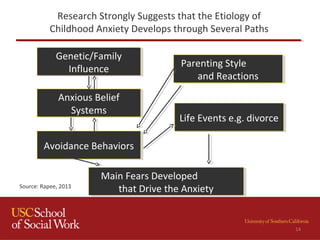
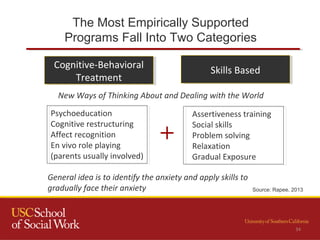
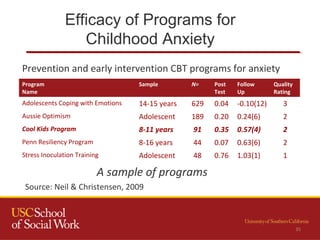
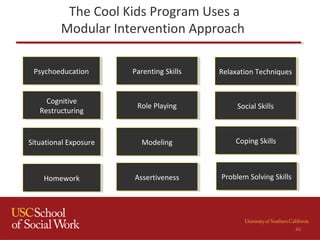

This document provides an overview of childhood anxiety disorders, with a focus on social anxiety disorder. It discusses the prevalence and impact of childhood anxiety, risk factors, theories of development, and symptoms. The document also reviews evidence-based treatments, particularly the Cool Kids cognitive-behavioral therapy program, which uses modules like psychoeducation, cognitive restructuring, relaxation techniques, and exposure. It emphasizes the importance of assessment, cultural considerations, and addressing comorbidities and family factors to achieve positive treatment outcomes.



















![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)















































