

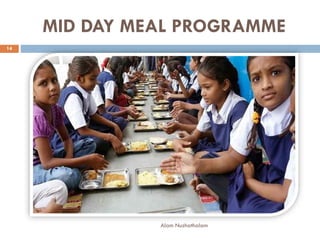


The document outlines various child welfare services in India, particularly through the Integrated Child Development Services (ICDS) program, aimed at supporting the health and nutrition of young children and mothers. It details the objectives, services, and impacts of programs like the Mid Day Meal and Anganwadi initiatives, which focus on improving children's health, education, and overall development. Additionally, it describes different types of child care options and the New Parent Support Program, which assists new parents in creating nurturing environments for their children.





































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







