Downloaded 33 times


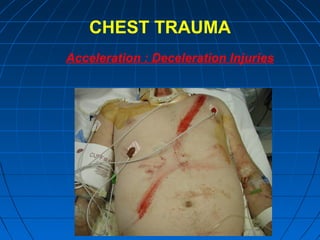

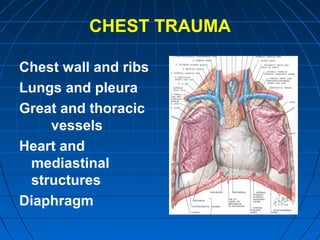
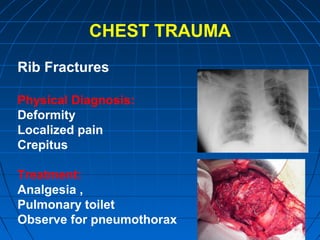
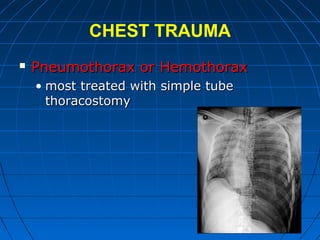
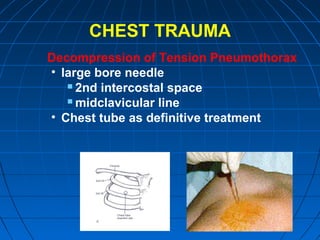

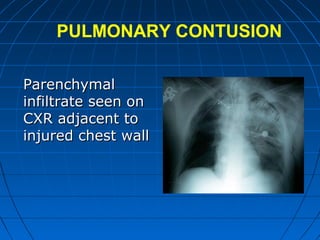
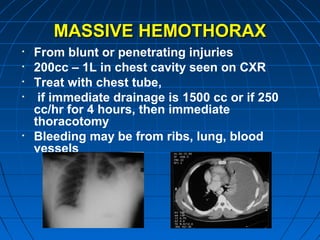
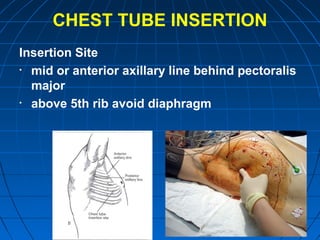
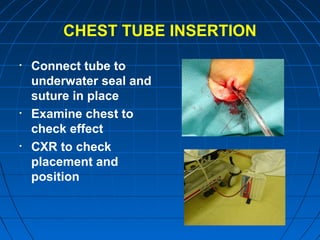

This document discusses chest trauma, including the different mechanisms of injury from blunt or penetrating sources. It describes common injuries such as rib fractures, pneumothorax, hemothorax, and pulmonary contusions. The initial management focuses on the ABCs and identifying life-threatening conditions like tension pneumothorax or cardiac tamponade. Specific injuries like flail chest require pain control, pulmonary therapy, or ventilator support. Radiologic tests help with diagnosis, and conditions may require chest tube insertion or surgery.