Cervical sympathetic block
Diagnostic:
◦ To determine if the pain is sympathetically mediated or not.
Prognostic:
◦ To determine if neurolysis or surgical sympathectomy could be beneficial
4.
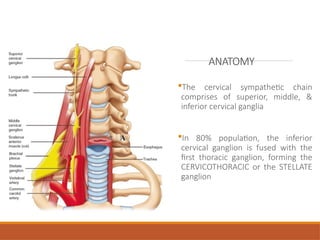
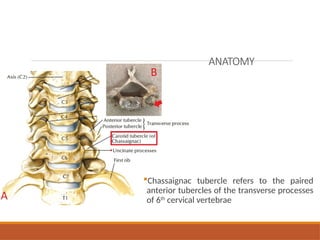
ANATOMY
The cervical sympatheticchain
comprises of superior, middle, &
inferior cervical ganglia
In 80% population, the inferior
cervical ganglion is fused with the
first thoracic ganglion, forming the
CERVICOTHORACIC or the STELLATE
ganglion
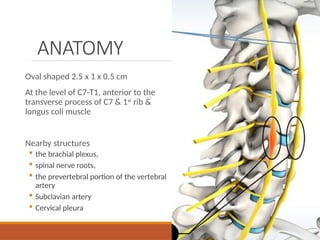
ANATOMY
Oval shaped 2.5x 1 x 0.5 cm
At the level of C7-T1, anterior to the
transverse process of C7 & 1st
rib &
longus coli muscle
Nearby structures
the brachial plexus,
spinal nerve roots,
the prevertebral portion of the vertebral
artery
Subclavian artery
Cervical pleura
7.
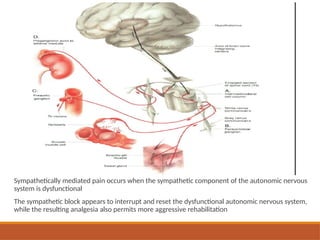
Sympathetically mediated painoccurs when the sympathetic component of the autonomic nervous
system is dysfunctional
The sympathetic block appears to interrupt and reset the dysfunctional autonomic nervous system,
while the resulting analgesia also permits more aggressive rehabilitation
8.
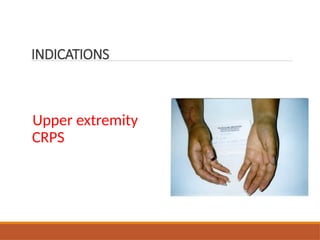
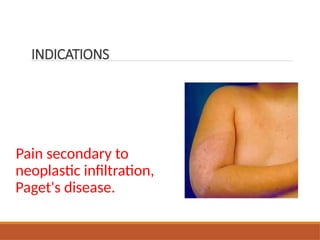
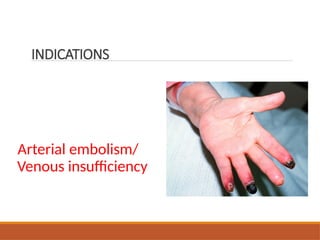
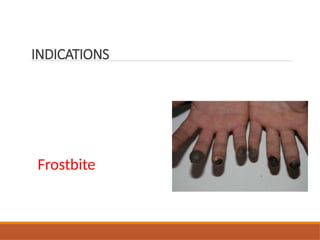
INDICATIONS
Most common indication- sympathetically mediated pain
Less common indications
◦ VT and electrical storm
◦ Hyperhidrosis
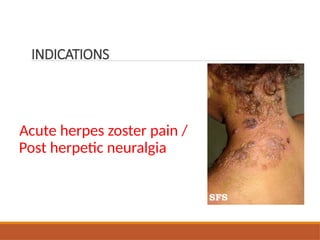
◦ Postherpetic neuralgia
◦ Ménière disease
◦ Accidental intra arterial injection of intravenous medications,
◦ Frost bite
◦ Angina pectoris
◦ Hot flashes and
◦ Posttraumatic stress disorders.
◦ Raynauds syndrome
9.
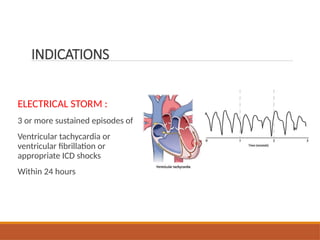
ELECTRICAL STORM :
3or more sustained episodes of
Ventricular tachycardia or
ventricular fibrillation or
appropriate ICD shocks
Within 24 hours
INDICATIONS
SURFACE LANDMARK TECHNIQUE
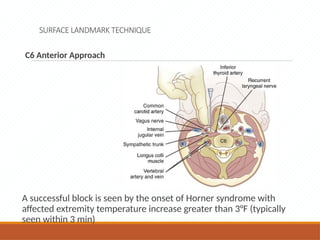
C6Anterior Approach
A successful block is seen by the onset of Horner syndrome with
affected extremity temperature increase greater than 3°F (typically
seen within 3 min)
19.
SURFACE LANDMARK TECHNIQUE
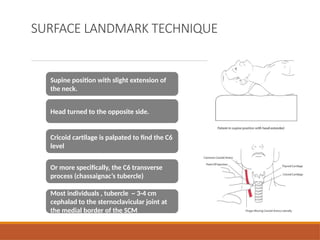
Supineposition with slight extension of
the neck.
Head turned to the opposite side.
Cricoid cartilage is palpated to find the C6
level
Or more specifically, the C6 transverse
process (chassaignac’s tubercle)
Most individuals , tubercle ~ 3-4 cm
cephalad to the sternoclavicular joint at
the medial border of the SCM
21.
SURFACE LANDMARK
TECHNIQUE
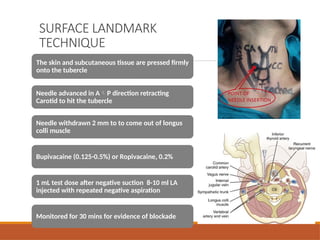
The skinand subcutaneous tissue are pressed firmly
onto the tubercle
Needle advanced in AP direction retracting
Carotid to hit the tubercle
Needle withdrawn 2 mm to to come out of longus
colli muscle
Bupivacaine (0.125-0.5%) or Ropivacaine, 0.2%
1 mL test dose after negative suction 8-10 ml LA
injected with repeated negative aspiration
Monitored for 30 mins for evidence of blockade
22.
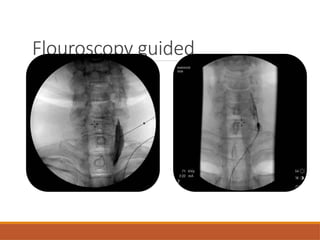
FLOUROSCOPY GUIDED
Landmarks andpatient positioning similar to blind technique
Bony delineation better – fluoroscopy
Soft tissues including vascular structures -ultrasound
Both the C6 transverse process approach and the C7 anterior
paratracheal approach can be done
Contrast to confirm appropriate needle placement
◦ Proper facial plane- local spread of contrast between the tissue planes both
cephalad and caudad.
◦ Striated appearance – Intramuscular
◦ Intravascular injection -immediate dissipation of dye
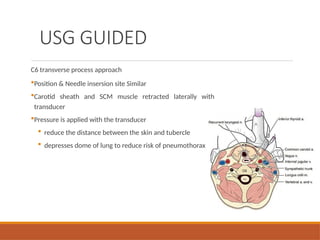
USG GUIDED
C6 transverseprocess approach
Position & Needle insersion site Similar
Carotid sheath and SCM muscle retracted laterally with
transducer
Pressure is applied with the transducer
reduce the distance between the skin and tubercle
depresses dome of lung to reduce risk of pneumothorax
25.
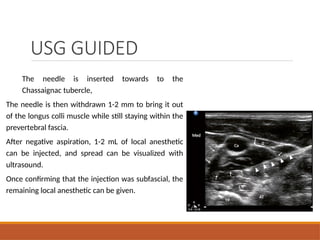
USG GUIDED
The needleis inserted towards to the
Chassaignac tubercle,
The needle is then withdrawn 1-2 mm to bring it out
of the longus colli muscle while still staying within the
prevertebral fascia.
After negative aspiration, 1-2 mL of local anesthetic
can be injected, and spread can be visualized with
ultrasound.
Once confirming that the injection was subfascial, the
remaining local anesthetic can be given.
26.
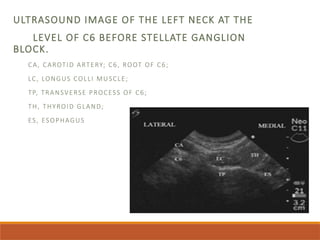
ULTRASOUND IMAGE OFTHE LEFT NECK AT THE
LEVEL OF C6 BEFORE STELLATE GANGLION
BLOCK.
CA, CAROTID ARTERY; C6, ROOT OF C6;
LC, LONGUS COLLI MUSCLE;
TP, TRANSVERSE PROCESS OF C6;
TH, THYROID GLAND;
ES, ESOPHAGUS
27.
C7 Anterior Approach
Nearlyidentical to the C6 approach.
Performed with USG or fluoroscopy - anatomical landmarks are more difficult to identify
because the C7 vertebra has only a vestigial tubercle that is not readily palpable.
Risk of pneumothorax and vertebral artery injury is higher.
Advantages
◦ Needle is closer in proximity to ganglion
◦ A smaller volume of LA agent with more reliable and consistent blockade.
◦ Particularily usefull - failed blockade at the c6 level.
An oblique C7 fluoroscopic approach targeting the junction between the uncinate process
and the vertebral body is described in an effort to decrease those risks.
Lateral approach (USG Guided) also described
28.
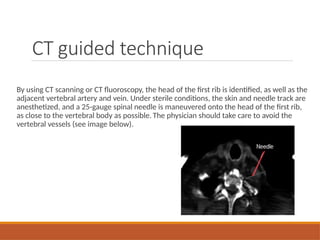
CT guided technique
Byusing CT scanning or CT fluoroscopy, the head of the first rib is identified, as well as the
adjacent vertebral artery and vein. Under sterile conditions, the skin and needle track are
anesthetized, and a 25-gauge spinal needle is maneuvered onto the head of the first rib,
as close to the vertebral body as possible. The physician should take care to avoid the
vertebral vessels (see image below).
29.
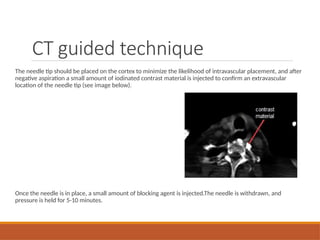
The needle tipshould be placed on the cortex to minimize the likelihood of intravascular placement, and after
negative aspiration a small amount of iodinated contrast material is injected to confirm an extravascular
location of the needle tip (see image below).
Once the needle is in place, a small amount of blocking agent is injected.The needle is withdrawn, and
pressure is held for 5-10 minutes.
CT guided technique
30.
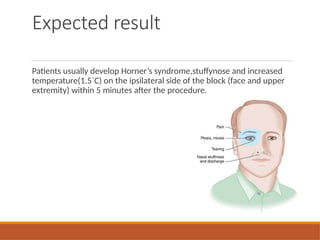
Expected result
Patients usuallydevelop Horner’s syndrome,stuffynose and increased
temperature(1.5`C) on the ipsilateral side of the block (face and upper
extremity) within 5 minutes after the procedure.
SUMMARY
Stellate ganglion blockis useful to denervate sympathetic component involved in upper
limb,head and neck disease conditions.
Careful evaluation of sympathetic involvement in disease process should be done before
deciding to perform block.
Blocking agent type, dose and subsequent blocks should be decided on the basis of
response to primary block.
After even successful stellate ganglion block patient should be monitored for side
effects.
#4 Chassaignac tubercle refers to the paired anterior tubercles of the transverse processes of 6th cervical vertebrae
#5 It separates carotid artery from the vertebral artery
Serves as important landmark wrt performing regional anasthesia such as brachial plexus and cervical plexus block & is a firm structure against which carotid massage can be performed
#7 The sympathetic nervous system (SNS) directly controls involuntary human homeostatic activities
The involuntary system controls numerous body functions such as sweating, the functions of the intestines and internal organs, dilation and contracting of the pupils in the eye, and blood flow through various tissues and has a major role in neuropathic, vascular, and visceral pain
#8 3 or more sustained episodes of
Ventricular tachycardia or ventricular fibrillation or appropriate ICD shocks
Within 24 hours
#22 With image guidance:
Anterior paratrecheal approach at C6 level
Anterior paratrecheal approach at C7 level
#25 Ultrasonographic image of the neck at C6 following injection of local anesthetic. The needle was indicated by solid arrows and the local anesthetic was outlined by the line arrows.
#28 Computed tomography fluoroscopic image shows the correct placement of a 25-gauge needle on the head of the first rib.
#29 Contrast material has been injected to confirm the extravascular location of the needle tip (same patient as in image above).
































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
