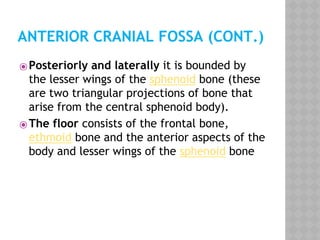
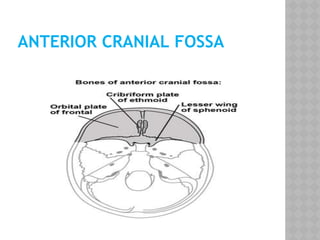
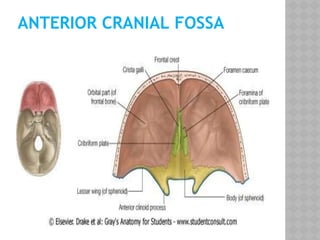
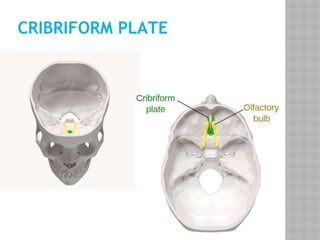
The anterior cranial fossa is the highest and most anterior of the three fossae of the internal skull. It is bounded by the frontal bone anteriorly and laterally, the sphenoid bone posteriorly and medially, and the lesser wings of the sphenoid bone posteriorly and laterally. It contains the inferior and anterior parts of the frontal lobes and important structures like the cribriform plate and crista galli. Injuries and tumors in this region can impact smell, vision, eye movement and cause CSF leaks. Both endoscopic and open craniotomy surgical approaches are used to access the anterior cranial fossa.