Downloaded 1,630 times
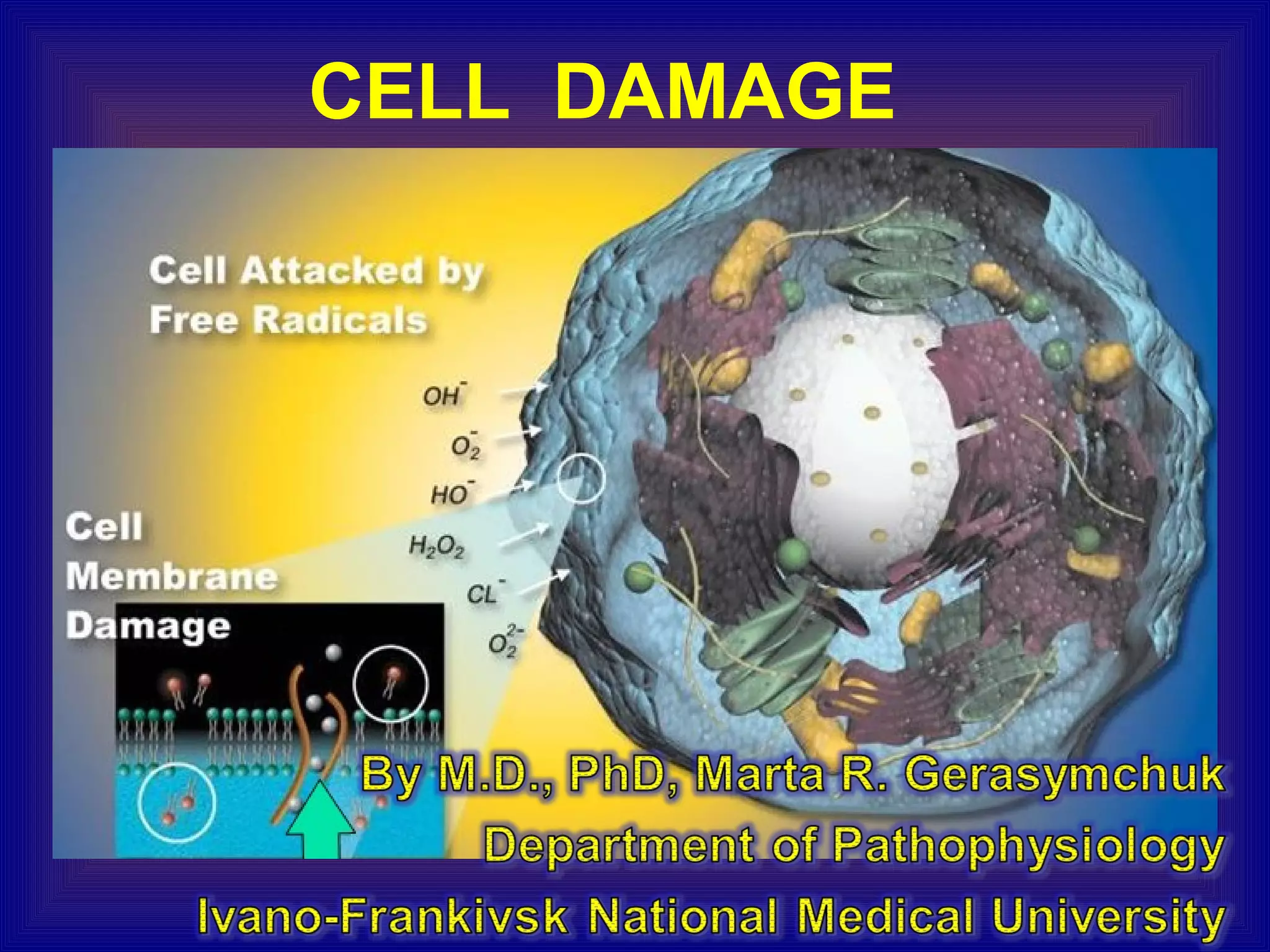





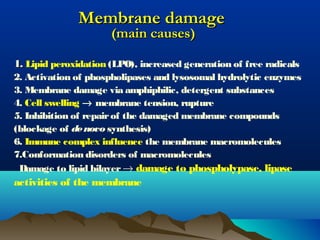
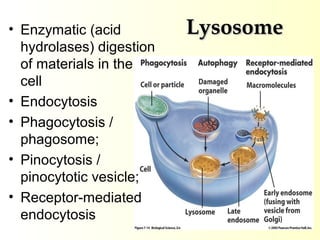
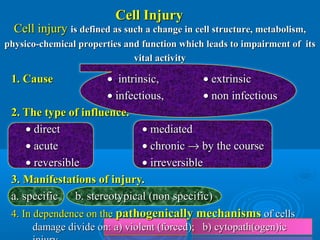


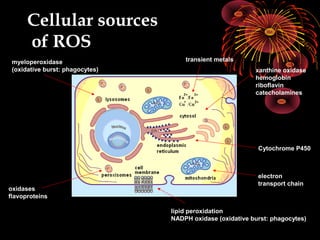
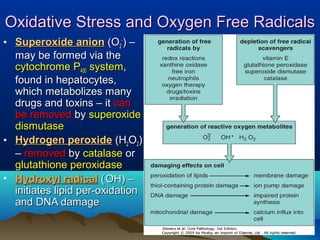
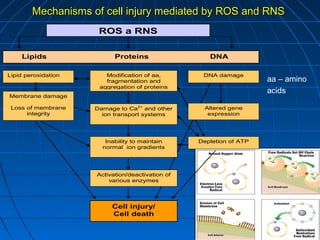
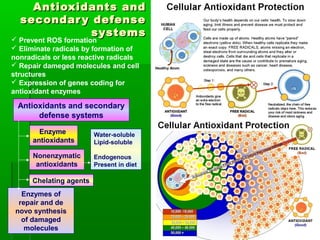
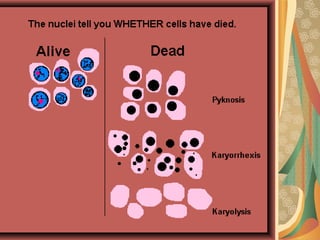
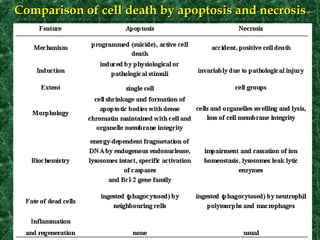
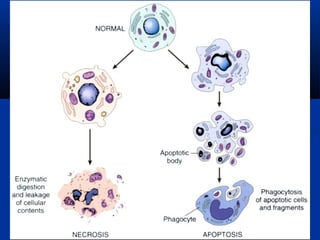



The document outlines classroom etiquette rules, including the prohibition of electronic devices and tobacco, while promoting cleanliness and respect towards others. It also discusses the etiology of diseases linked to atmospheric pressure changes and barotrauma, detailing the necessary knowledge and practical skills for analyzing disease causes. Additionally, the document covers cell injury mechanisms, types, and classifications, emphasizing cellular responses to various environmental stresses.































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








