Download to read offline


![The name of the previous and
future disciplines
The receiving of the skills
1. Histology
2. Biochemistry
3. Pphysiology
4. Internal medicine
5. Haemathology
6. Surgical stomatology
Scheme of erythropoiesis.
Quantitative parameters of red blood.
Technique of erythrocytes account.
Technique of determination of the hemoglobin
content.
Technique of determination of a colour index.
5. The advices for student
Normal content of erythrocytes (red blood cells - RBC) and hemoglobin in blood:
Erythrocytes: M — 4.0-5.0·1012
/l; F — 3.9-4.7·1012
/l; Newborn: 5-6·1012
/l
Hemoglobin (Hb): M - 135-160 g/l; F - 120-140 g/l;
Mean corpuscular hemoglobin (MCH) = [Hb] / RBC count: 0.85-1.15
Reticulocytes: 2-10 % (of total erythrocyte number)
Erythrocytes sedimentation rate (ESR): M - 2-10 mm/h; F - 2-15mm/h
Hematocrit: Adults: M - 40-48%; F - 36-42%; Newborn: 45-54%
Size of erythrocyte- 7-8 µm
Life span of erythrocyte - 120 days
Maturation of erythrocyte - 3 days
Total amount of erythrocytes in blood of adults - 25·1012
/l
Destroyed and formed daily up to 1% of total amount of erythrocytes (210 billion).
Iron in blood 8.53-28.06 µmol/l
Ferritin, serum in men 96±7.63 µg/l, in women 45.5±4.58 µg/l.
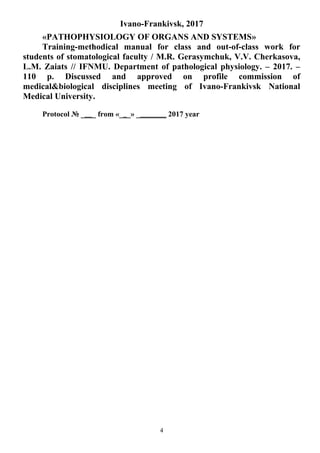
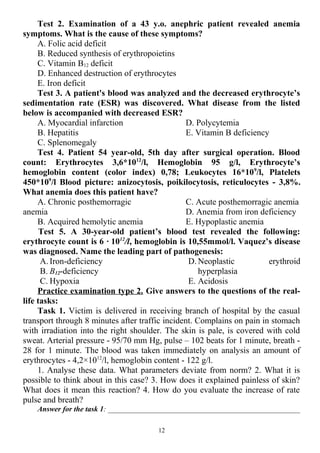
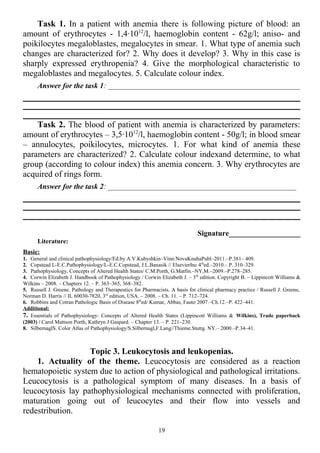
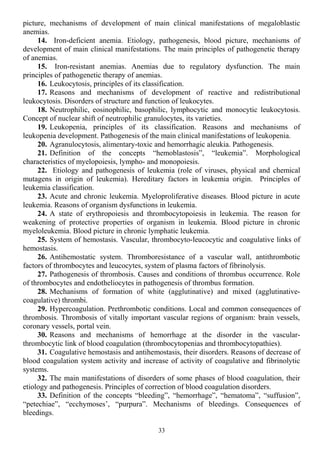
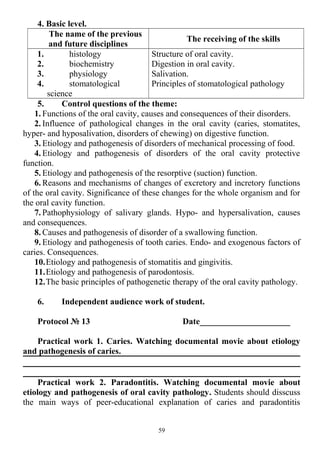
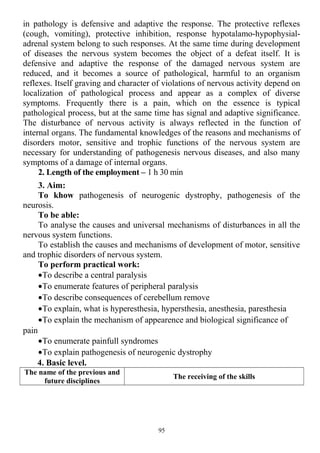
5.2. Practical part: Manual Cell
Counting (by microscope)
Neubauer counting chamber from above with
cover slip. Notice the two counting grids which are
recognized as crosses.
Schematic representation of the Neubauer counting
chamber's counting grid: blue = area of the leukocyte count
red = areas of the erythrocyte and platelet counts
Since blood cells are counted per unit volume (per
liter), it is vital that the volume of blood, in which the
cells are counted, corresponds to a known quantity. This
makes the Neubauer
counting chamber a
useful method. A
special objective slide
on which two 3 x 3
mm long counting
grids were engraved
comprises the Neubauer counting chamber.
8](https://image.slidesharecdn.com/2017metod-180819004340/85/Metod-stomat-f-ty-1st-semester-book-Module-2-8-320.jpg)






![5. What is leukopenia? Classification of the leukopenia.
6. Etiology of the leukopenia.
7. The mechanisms of leucopenia.
8. What is aleukia, agranulocytosis?
9. Blood picture under the leukopenia.
10. Leucocyte degeneration in blood.
11. Hereditary WBC abnormalities.
7. Students’ practical activities
Protocol № 3 Date_____________________
Experimental work 1. Count up a leucocytic formula (leucogram) at an
abscess. To prepare the stroke of blood, taken from the vein of ear of rabbit and
to paint it after Pappengeym. See the stroke under a immersion increase. The
stroke of blood is mentally divided into four fields, conducting the lines which
are perpendicular one to one through the center of stroke. Count up in every
field 25 leucocytes, moving a stroke on the broken line. Count up separate types
of leucocytes using a meter.
Formula: LG
А
L
АА
/
20
/10
20
10
11600
204000 96
=•=•
•
••
,
А – amount of leucocytes in 100 big squares; 1600 – amount of small squares; 4000
1
-
a volume of small square is in microliter; 20 - is a degree of breeding of blood; 106
- is a
multiplier for the count of amount of leucocytes in CI units; G - giga = 109
Conclusion:__________________________________________________________
Experimental work 2. Define the index of nuclear change.
The index of nuclear change of neutrophiles is determined after a formula:
S
BYМ
%
%%% ++
where
M – mielocytes B – band [stab] neutrophiles
Y – young neutrophiles S – segmented [polynuclear] neutrophiles.
Index of nuclear exchange in norm 0,6-0,8
Conclusion:__________________________________________________________
____________________________________________________________________
8. Practice Examination.
22](https://image.slidesharecdn.com/2017metod-180819004340/85/Metod-stomat-f-ty-1st-semester-book-Module-2-22-320.jpg)

![necessary to mark that the therapy of leucosis mainly pathogenetic. The
deepening of our submissions about separate chains of pathogenesis will
promote perfecting of purposeful treatment.
2. Length of the employment – 1h 30 min.
3. Aim:
To know: leukemia –is a disease of tumor nature, originating from blood
cells with initial affection of the bone marrow.
To be able: to analyse of the pathogenesis and blood data under acute and
chronic leukemia.
To perform practical work: to analyse of the pathogenesis of the
leukemia. Oncogenic viruses, ionizing radiation and chemical substances cause
mutation of genes or epigenomic disturbance of regulation of multiplication and
maturation of hematopoietic cells of the II-nd and III-rd levels. Leukemia
viruses can cause such chromosomal translocation that result in transmission of
the oncogenes, localized in chromosomes, to the part of genome where they can
be activated
4. Basic level.
The name of the previous
and future disciplines
The receiving of the skills
1. histology
2. biochemistry
3. physiology
4. oncology
5. surgical
stomatology
Scheme of hematopoisis.
Morphological features of leucocytes.
Leucocytic formula of blood.
Function of leucocytes.
5. Control questions of the theme:
1. Determination and general definition of leucosis. Classification of
leucosis is after motion and morphological signs.
2. Modern theories of origin of leucosis: role of viruses, ionizing radiation,
chemical matters, inherited anomalies. Tumor nature of leucosis. Basic displays
of tumor progression.
3. Features of hemopoiesis, picture of peripheral blood, leucogram at an
acute myeloleucosis [myeloleukemia].
4. Features of hemopoiesis, picture of blood at chronic myeloleucosis.
5. Picture of blood, leukogram at an acute lympholeucosis [lymphatic
leukemia].
6. Picture of blood, leukogram at a chronic lympholeucosis.
7. A mechanism of development of anemia at acute and chronic leucosis.
8. Violation of reactivity of organism is at leucosis.
9. A role of the inherited anomalies is in development of leucosis.
6. Independent audience work of student
25](https://image.slidesharecdn.com/2017metod-180819004340/85/Metod-stomat-f-ty-1st-semester-book-Module-2-25-320.jpg)



![3. Aim: To form for students the modern knowledge of reasons and
mechanisms of violation thrombocyte-vascular and coagulative hemostasis, to
design these processes in an experiment on animals with the purpose of
cognition of reasons and terms of their origin, mechanisms of development,
consequences and value of these processes in pathology of man.
To khow:
- etiologic factors which predetermine violation of producing blood clots;
- basic phases of process of producing blood clots;
- reasons and mechanisms of origin of hemorrhagic diathesis;
- reasons and mechanisms of violation thrombocyte-vascular hemostasis;
- etiology and pathogenesis of disseminated intravascular clotting [DIC];
- inherited violations of blood clotting.
To be able:
- to explain the mechanisms of interrelation of basic factors of coagulative
and anticoagulative systems in the process of clotting;
- to reproduce violation of blood clotting in an experiment;
- to calculate prothrombin time [PT] and prothrombin index;
- to count up the amount of platelets in peripheral blood.
A task is to independent extracurricular work:
Modern presentations about coagulative and anticoagulative system of blood.
Mechanisms of the physiology blood clotting. Thrombosis as local violation of
circulation of blood.Stages of blood clotting.
To perform practical work: to analyse of the pathogenesis of the platelet
adhesion and aggregation.
4. Basic level.
The name of the previous and future
disciplines
The receiving of the skills
1. histology
2. biochemistry
3. physiology
4. internal medicine
5. haematology
Vesseles-thrombocytous and plasmatic factors,
which participate in coagulation of blood.
Stage of blood coagulation.
Significance ancoagulative and fibrinolytic
systems of blood.
5. Control questions of the theme:
1. What is hemostasis pathology. Classification of hemostasis pathology.
2. Normal hemostasis.
3. The classical coagulation cascade.
4. Virchow's triad in thrombosis.
5. Decreasing of blood coagulation ability.
6. Thrombocytopenia and thrombocytopathy.
7. Increasing of blood coagulation ability.
29](https://image.slidesharecdn.com/2017metod-180819004340/85/Metod-stomat-f-ty-1st-semester-book-Module-2-29-320.jpg)
![8. Generalized disseminated intravascular blood coagulation (DIC-
syndrome).
9. Hereditary disorders of coagulation.
6. Independent audience work of student
Protocol № 5 Date_____________________
Experimental work 1. Define prothrombin time [PT] for a dog with the
cirrhosis of liver. In advance oily solution of carbon tetrachloride is entered a
dog from the calculation of 4 ml per 1 kg of mass. Before lesson for a dog take
4,5 ml of blood, add 0,5 ml of a 0,1% solution of oxalic sodium and spin, take
the plasma. In test tube pour 0,2 ml of plasma, warm up on an water bath at
38°N, add 0,2 ml warmed to a 38°N mixture from equal parts of thromboplastin
and 0,5% solution of calcium chloride. Carefully mix up a glass stick,
continuing to hold in a water bath. Calculate time from adding mixture to the
first signs of coagulation of plasma (in seconds).
Calculate the prothrombin indexes after formula: B
А
Х
•
=
100
, where A – time
of coagulation of control plasma (seconds); B – time of coagulation of
experimental plasma (seconds). A normal index of is equal 70-100%.
Conclusion
Experimental work 2. Count up the amount of thrombocytes for a
rabbit with radiation illness. Three days prior to lesson an animal is exposed
to the X-rays.
On the area of regional vein ears inflict a few drops of a 14% solution of
magnesium sulphate, prick a vein; carefully mix up blood a glass stick with
magnesia in correlation 2:10.
From the got mixture prepare a stroke, dye it after Pappengeym (to repaint
for the best visibility of trombocytes). A count is conducted under a immersion
increase in the narrowed eyeshot. Count up the amount of trombocytes on 1000
RBC.
Formula of calculation: 1000
АН
Х
•
= , where H – is an amount of platelets on
1000 RBC; A – is an amount of RBC;.Method of count of amount of RBC see
in previouse lesson.
Conclusion
30](https://image.slidesharecdn.com/2017metod-180819004340/85/Metod-stomat-f-ty-1st-semester-book-Module-2-30-320.jpg)





![hemodynamics at condition insufficiency of blood circulation. Study concepts
and essence of hypertrophy of myocardium, features of its metabolism,
mechanisms of compensation and decompensation.
To know:
- types of insufficiency of heart and principal reasons of their
development;
- heterometric and homeometric mechanisms of compensation of
insufficiency of heart;
- hypertrophy of myocardium, its stage, feature of the hypertrophied heart;
To be able:
- to explain changes in an organism at the condition insufficiency of blood
circulation;
- to determine character of compensate reactions of myocardium on
experimental model of acute insufficiency of heart (depending on the type of
loading on a heart), discover and explain changes which pass here.
A task is to independent extracurricular work:
1. Structure of heart, its valves, circles of blood circulation [systemic and
pulmonary].
2. Features of innervation, metabolism and bloodstream of heart.
3. Phases of cardiac cycle, their description.
4. Physiology law of the heart [Frank-Starling's law]
5. Systolic [stroke volume] and minute volume [cardiac output] of heart,
methods of their determination.
6. Processes of energy supply of cardiac muscle.
To perform practical work: To analyse the compensatory mechanisms
cardio-vascular diseases.
4. Basic level.
The name of the previous and
future disciplines
The receiving of the skills
1. histology
2. biochemistry
3. physiology
4. internal medicine
5. cardiology
6. intensive care
Histochemical structure of the myocardium. Specialities
of blood supply of heart. The main physiological features
of heart function. Principle of operation of the
electrocardiograph. Technique of record of an
electrocardiogram in three standard leads. Principal
components of an electrocardiogram.
5. Control questions of the theme:
1. Insufficiency of blood circulation: determination, classification.
2. The most widespread innate defects of heart. Mechanisms of
compensation.
3. Reasons and displays of acute cardiac insufficiency.
4. Pathogenesis of cardiac insufficiency at the overload of heart by the
39](https://image.slidesharecdn.com/2017metod-180819004340/85/Metod-stomat-f-ty-1st-semester-book-Module-2-39-320.jpg)



![electrocardiogram in three standard
leads.
Principal components of an
electrocardiogram.
5. The advices for students.
Classification of coronary heart disease.
There are 4 main types clinical manifestations of coronary heart disease.
1. Stenocardia (angina pectoris)
a) Stenocardia of the stress;
b) Stenocardia of the rest
2. Myocardial infarction
3. Intermediate variants
a) Acute focal myocardial dystrophy;
b) Small focal myocardial infarction
4. Indolence CHD
a) Silent (asymptomatic) CHD;
b) Atherosclerotical cardiosclerosis
6. Control questions of the theme:
1. Features of coronal circulation of blood and metabolism of cardiac
muscle.
2. Classification of coronary heart disease. CHD: determination, reasons
and terms of origin, form.
3. Ischemic heart disease. Definition of the notion, risk factors, mechanisms
of development
4. Sudden coronary death: reasons, mechanisms of origin.
5. Angina pectoris: classification, pathogenesis of displays.
6. Heart attack of myocardium: kinds, description of functional and
biochemical violations in a cardiac muscle, mechanisms of pain syndrome.
7. Mechanisms of origin of spasms of coronary vessels.
8. Complication of heart attack of myocardium. Pathogenesis of cardiogenic
shock.
9. Experimental models of heart attack of myocardium.
10. Dressler’s syndrome, hibernal myocardium, methods of diagnosis, main
manifestations (blood tests, coagulogramm, ECG, SCG.
11. Noncoronary damages of myocardium: reasons, mechanisms of
development.
12. Damage of pericardium. Cardiac [pericardial] tamponade: reasons,
displays, mechanisms of indemnification.
7. Independent audience work of student.
44](https://image.slidesharecdn.com/2017metod-180819004340/85/Metod-stomat-f-ty-1st-semester-book-Module-2-44-320.jpg)































![Practical skills for chapter
“Pathophysiology of endocrine and nervous system”.
1. Etiology and basic mechanisms of origin of endocrine diseases. Violations of direct
and feedback links in pathogenesis of dysregulative endocrine pathology.
2. Glandular and peripheral violations of endocrine function. Reasons and mechanism
of violations of biosynthesis, depositing and excretion of hormones. Violations of transport,
inactivation and reception of hormones.
3. Violation of function of hypothalamus and adenohypophysis. Etiology and
pathogenesis of basic displays.
4. Violation of function of hypothalamus and neurohypophysis. Etiology and
pathogenesis of basic displays. Hypopituitarism: it kinds, etiology and pathogenesis,
clinical displays.
5. Hypo(adreno)corticism, its forms. Etiology and pathogenesis of basic displays.
There are displays, which connect with disorders of secretion mineralo- and glucocorticoids
by adrenal glands.
6. Hyperfunction of adrenal glands. Primary and secondary hyperaldosteronism, its
kinds, mechanisms of displays. Adrenogenital syndrome syndrome: reasons and
mechanisms of development.
7. Pituitary [Cushing's] basophilism (disease) and Cushing's syndrome: etiology and
mechanisms of clinical displays.
8. Hyperthyroidism, its etiology and pathogenesis.
9. Hypothyroidism: forms, basic displays, etiology and pathogenesis.
10. Goiter, their kinds, etiology and pathogenesis, clinical displays.
11. A role of stress in pathology. Stages of stress, their pathogenesis. “Diseases of
adaptation”.
12. Insufficiency of function of parathyroid glands. Basic displays, etiology and
pathogenesis.
13. Hyperparathyroidism: etiology, pathogenesis of basic displays.
14. Hypergonadism and hypogonadism. Etiology and pathogenesis, basic displays in a
men and women.
15. Disorders of sensor function of nervous system. Violations of touch, term and
proprioception and nociception. Violations of conducting sensor information.
16. The pain, its kinds, reasons, mechanism of development. Analgetic [antinoceptive]
systems of organism.
17. Disorders of sensor function of cortex (sensitiveness). Neuroses: etiology,
pathogenesis, forms.
18. Disorders of motor function of nervous system. Paralysis, it kinds. Spinal shock.
19. Disorders of trophic function of nervous system. Neuro-dystrophic process.
Structural, functional and biochemical changes in denervated organs and tissues.
20. Etiology and pathogenesis of damages of CNS. Disorders of brain blood
circulations. Strokes and edema of brain.
21. The role of glia and blood-brain [hematoencephalic] barrier in development of
pathological processes in CNS. Intracranial hypertension.
109](https://image.slidesharecdn.com/2017metod-180819004340/85/Metod-stomat-f-ty-1st-semester-book-Module-2-109-320.jpg)


The document contains: 1. An introduction and overview of the training manual. 2. A calendar plan of practical classes and lectures on pathophysiology topics. 3. Detailed instructions and learning objectives for topics related to the pathophysiology of blood, circulation, respiration, digestion, liver/kidneys, endocrine and nervous systems.