Catheters are thin, flexible tubes that can be inserted into body cavities, ducts, or vessels. They are made from biocompatible materials like silicone, latex, or polymers. Catheters have various uses including draining fluids, delivering medications, or providing access for surgical instruments. Common types of catheters include urethral catheters, which drain the bladder; central venous catheters, which provide long-term intravenous access; and peripheral venous catheters for short-term intravenous access. Proper insertion and maintenance of catheters is important to provide benefits while avoiding complications like infection, injury, or blockage.









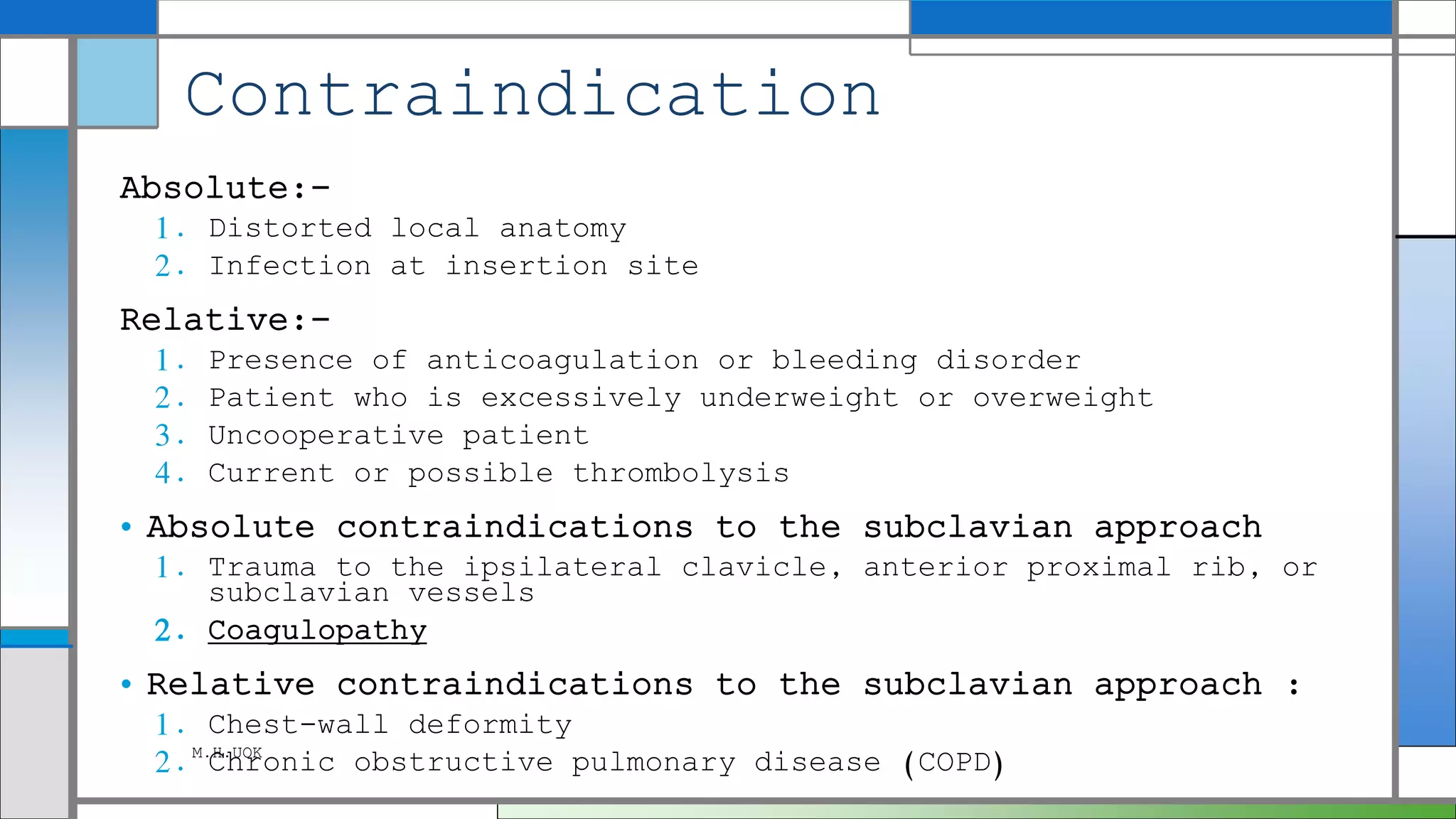
![Contraindications
• traumatic injury to the lower urinary
tract (eg, urethral tear).
• This condition may be suspected in male
patients with a pelvic or straddle-type
injury.
• Signs that increase suspicion for injury
are a high-riding or boggy prostate,
perineal hematoma, or blood at the meatus.
When any of these findings are present in
the setting of possible trauma,
• a retrograde urethrogram should be
performed to rule out a urethral tear prior
to placing a catheter into the bladder. [2]
M.H.UOK](https://image.slidesharecdn.com/catheters-180115001412/75/Catheters-14-2048.jpg)