Cardiac arrhythmia
- Termarrhythmia refers to disturbance in rate , regularity, site
of origin, or conduction of cardiac electrical impulse.
- It may cause sudden death, syncope, heart failure, chest pain,
dizziness, palpitation, or no symptoms at all.
- Why they happen – HIS DEBS
Hypoxia
Ischemia
Sympathetic stimulation
Drugs
Electrolyte disturbance
Bradycardia
Stretch
3.
There are FOURbasic types of arrhythmia :-
(a) Electrical activity follows the usual conduction pathway –
Arrhythmia of sinus origin
(b) Electrical activity originates elsewhere than the sinus node –
Ectopic rhythms
(c) Electrical activity originates in SA node follows usual
pathway but encounters blocks and delays
Conduction Blocks
(d) Electrical activity follows the accessory conduction pathway
and bypass the normal
Pre excitation Syndrome
4.
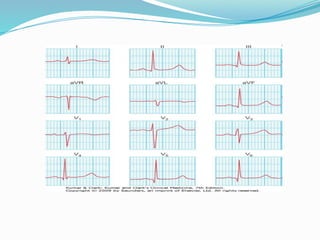
Sinus node function
-Thecardiac pacemaker is the sinus node, it depolarizes
spontaneously.
-The sinus node is under the influence of the autonomic
nervous system, with a parasympathetic predominance
6.
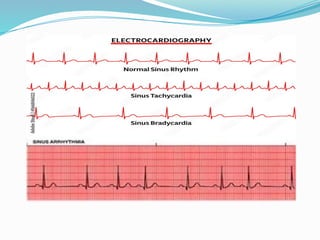
Sinus Arrhythmias
-Change inrhythm during respiration, due to
fluctuation in autonomic tone during breathing, with
inspiration heart rate quickens, and on expiration the
heart rate falls. This is normal variation
Sinus bradycardia
- A sinus rate < 60 b/min
It is asymptomatic, unless rate is very slow.
Sinus tachycardia
- A sinus rate > 100 b/min.
(a) Arrhythmia of sinus origin
8.
Sinus bradycardia :
Extrinsiccauses
- Hypothermia, Hypothyroidisim, Cholestatic jaundice and raised
intracranial pressure, dyselectrolytemia.
- Neurally mediated syndromes- they include Carotid sinus
syndrome, Vaso vagal syncope , Besold -Jarisch Reflex which cause
both bradycardia and reflex peripheral vasodilatation With
hypotension
- Drugs like beta-blockers , non dihyropyridine CCB, digitalis
9.
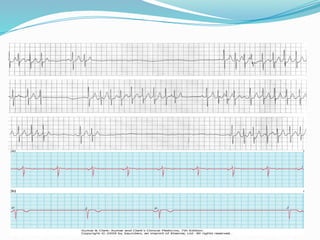
Intrinsic causes
- Acuteischaemia and infarction of the sinoatrial nodal artery as
a complication of myocardial infarction
- Chronic degenerative changes e. g. ( sick sinus syndrome).
- Which is caused by
Idiopathic fibrosis of the sinus node,
Ischaemic heart disease,
Cardiomyopathy and
Myocarditis
It is characterized by episodes of sinus bradycardia or sinus
arrest, alternating with paroxysmal atrial tachycardia
(tachy-brady syndrome)
11.
Treatment
Sinus bradycardia :-Identify and treat any extrinsic cause
Temporary pacing for reversible causes.
Permanent pacing for chronic degenerative
causes.
Sick sinus syndrome :- Permanent pacing with anti
arryhthmic drugs or ablation
therapy for tachycardia element.
Vasovagal attacks :- Elastic stockings, Drugs like beta- blockers
or disopyramide were tried but did not show
fruitful results
12.
- Intrinsic -sinus node dysfunction is rare
- Extrinsic
Acute causes like :-
Exercise, Emotion, Pain, Fever, Infection,
Acute Heart Failure, Acute Pulmonary
Embolism, And Hypovolaemia.
Chronic causes like:-
Pregnancy, Anaemia, Hyperthyroidism
And Catecholamine Excess.
Causes of sinus tachycardia
13.
(b) Ectopic rhythms-
Mechanisms
1.Enhanced Automaticity – Impulse formation
2. Reentry – Impulse Transmission
Four questions to be asked
Are normal P wave present?
Are the QRS complex Narrow Or Wide?
What is relationship between P wave and QRS complex?
Is the rhythm regular or irregular?
14.
It include
Atrial andJunctional Premature Beats
Atrial fibrillation
Atrial flutter
Multifocal atrial tachycardia
Atrial ectopic tachycardia ( Paroxysmal atrial tachycardia -PAT)
PSVT / AV Nodal Reentrant tachycardia
Ectopic Supra ventricular Arrhythmias
15.
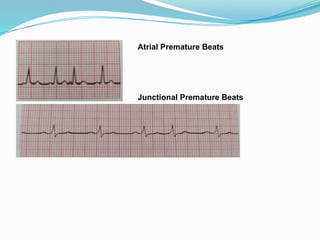
Atrial and JunctionalPremature Beats
Atrial premature beats - मेरे पास P wave हैं
Junctional Premature Beats - मेरे पास गाड़ी है, बंगला हैं, नौकर है,
…
तुम्हारे पास क्या है ?
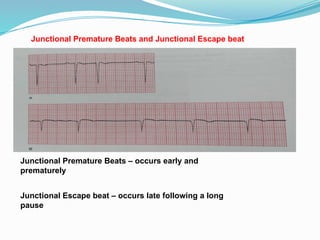
Junctional Premature Beatsand Junctional Escape beat
Junctional Premature Beats – occurs early and
prematurely
Junctional Escape beat – occurs late following a long
pause
18.
Atrial fibrillation
- Itis a common arrhythmia, may occur in paroxysmal
form in young patients.
- Of the many causes ,the classical are RHD, alcohol
intoxication, thyrotoxicosis, hypertension and heart
failure are common causes.
- AF consist of continuous, rapid (300-600 per min.)
activation of the atria by multiple re-entry wavelets
21.
Symptoms and signs
-Asymptomatic
- Palpitation
- Dyspnoea
- Syncope
- Chest pain
- Worsening in a previous
cardiac complaint
- On examination : Irregularly irregular pulse
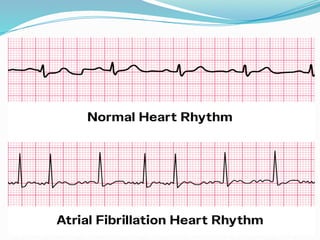
- ECG
Fine oscillation of the baseline – undulating baseline
No clear P wave
QRS rhythm is rapid and irregular
Ventricular rate - Variable
22.
Management
- Treat provokingcause
- Control ventricular rate by drugs ;-
Digoxin monotherapy or in combination with
Calcium-channel blockers/ Beta-blockers
- Cardioversion by DC shock (120 – 200 joules) or by
drugs ;-
Class Ic agents (e.g.flecanaide) for patients with no significant heart
disease
ClassIII agents ( e.g. amiodarone) for patients with significant heart
disease
- Anticoagulation
Note - Patients are typically given blood-thinning medication for several
weeks before the procedure to prevent the formation of blood clots in the
heart, which could lead to a stroke if dislodged by the shock.
Transesophageal echocardiography (TEE):
A TEE may be performed to check for existing blood clots before the
23.
Anticoagulation
The CHA₂DS₂-VASc ScoreComponents
•C: ongestive heart failure or left ventricular dysfunction: 1
point
•H: ypertension: 1 point
•A: ge 75 years:
≥ 2 points
•D: iabetes mellitus: 1 point
•S: troke/Transient Ischemic Attack (TIA)/Thromboembolism:
2 points
•V: ascular disease (e.g., history of myocardial infarction,
peripheral artery disease): 1 point
•A: ge 65–74 years: 1 point
•S: ex category (female): 1 point
24.
How It's Used
1.Calculatethe score: Sum the points from the relevant risk
factors for each patient.
2.Risk Stratification: The total score stratifies the patient's risk of
stroke.
•Low Risk: Generally a score of 0 (men) or 1 (women) is
considered low risk.
•High Risk: Higher scores indicate increased risk.
3.Guide Treatment: The score helps clinicians decide whether to
initiate or change anticoagulant therapy to prevent a stroke. For
instance, guidelines often suggest oral anticoagulation for men
with a CHA₂DS₂-VASc score of 2 or more and for women with a
score of 3 or more.
25.
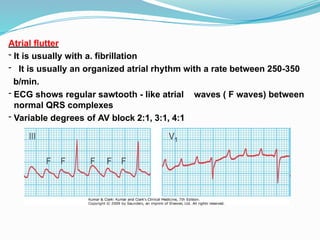
Atrial flutter
- Itis usually with a. fibrillation
- It is usually an organized atrial rhythm with a rate between 250-350
b/min.
- ECG shows regular sawtooth - like atrial waves ( F waves) between
normal QRS complexes
- Variable degrees of AV block 2:1, 3:1, 4:1
26.
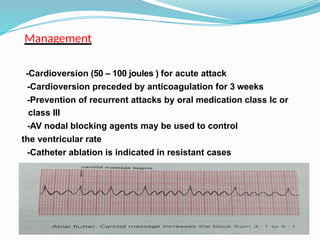
Management
-Cardioversion (50 –100 joules ) for acute attack
-Cardioversion preceded by anticoagulation for 3 weeks
-Prevention of recurrent attacks by oral medication class Ic or
class III
-AV nodal blocking agents may be used to control
the ventricular rate
-Catheter ablation is indicated in resistant cases
27.
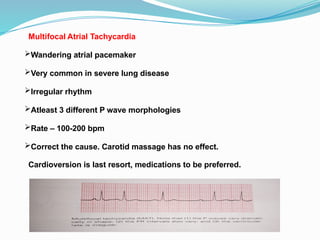
Multifocal Atrial Tachycardia
Wanderingatrial pacemaker
Very common in severe lung disease
Irregular rhythm
Atleast 3 different P wave morphologies
Rate – 100-200 bpm
Correct the cause. Carotid massage has no effect.
Cardioversion is last resort, medications to be preferred.
28.
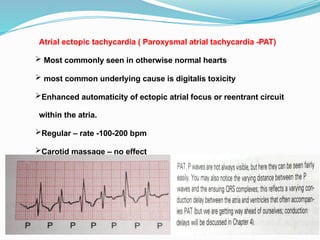
Atrial ectopic tachycardia( Paroxysmal atrial tachycardia -PAT)
Most commonly seen in otherwise normal hearts
most common underlying cause is digitalis toxicity
Enhanced automaticity of ectopic atrial focus or reentrant circuit
within the atria.
Regular – rate -100-200 bpm
Carotid massage – no effect
29.
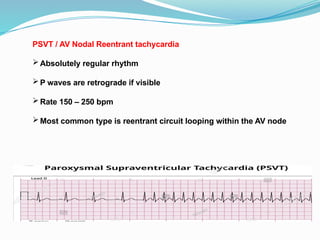
PSVT / AVNodal Reentrant tachycardia
Absolutely regular rhythm
P waves are retrograde if visible
Rate 150 – 250 bpm
Most common type is reentrant circuit looping within the AV node
30.
Symptoms of PSVT
-Palpitation, rapid regular , with abrupt onset and sudden
termination, which occur spontaneously or be precipitated
by alcohol, coffee, or just sheer excitement.
- Anxiety, dizziness, dyspnoea, central chest pain, polyuria
weakness and Syncope
31.
Acute management
- Patientwith haemodynamic instability (hypotension,
pulmonary oedema ) require emergency cardioversion
(50- 100 joules)
- If the patient is stable vagal manoeuvres , including
right carotid massage ,Valsalva manoeuvre and facial
immersion in cold water can be used also.
- If no effect then IV adenosine ( 6 mg. ) it acts within
seconds causing abrupt termination, the side effect
include bronchospasm, flushing, chest pain it is
contraindicated in asthmatics.
- Verapamil 5-10 mg. i.v. over 10 minutes, diltiazem or
beta-blokers
33.
Long-term management
Referfor electrophysiological evaluation
Drugs like verapamil, diltiazem, beta- blockers,
flecainide, sotalol, and amiodarone.
Catheter ablation
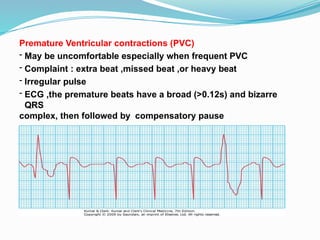
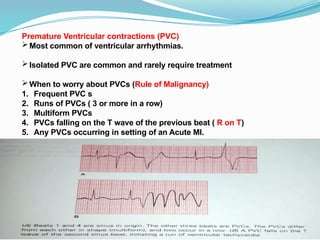
Premature Ventricular contractions(PVC)
- May be uncomfortable especially when frequent PVC
- Complaint : extra beat ,missed beat ,or heavy beat
- Irregular pulse
- ECG ,the premature beats have a broad (>0.12s) and bizarre
QRS
complex, then followed by compensatory pause
37.
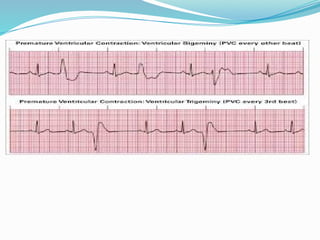
Premature Ventricular contractions(PVC)
Most common of ventricular arrhythmias.
Isolated PVC are common and rarely require treatment
When to worry about PVCs (Rule of Malignancy)
1. Frequent PVC s
2. Runs of PVCs ( 3 or more in a row)
3. Multiform PVCs
4. PVCs falling on the T wave of the previous beat ( R on T)
5. Any PVCs occurring in setting of an Acute MI.
Normal heart ventriculartachycardia
- It is usually benign
- It is idiopathic and monomorphic
- Excellent long- term prognosis
- If symptomatic ,treatment with beta-
blockers ,verapamil or catheter ablation
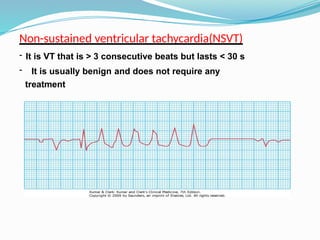
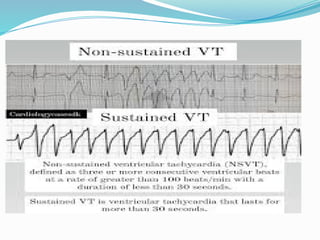
40.
Life- threatening ventriculartachyarrhthmia –
This life threatening condition with haemodynamic instability
(e.g. syncope, hypotension ) presents as
- Sustained ventricular tachycardia
- Ventricular fibrillation
41.
Sustained ventricular tachycardia
-It last (>30 s) causing pre- syncope (dizziness) syncope,
hypotension and cardiac arrest.
- On examination pulse rate between 120-220 b.p.m. with variable
degrees of atrio-ventricular dissociation ( cannon a wave in JVP)
ECG shows rapid ventricular rhythm with broad (0.12s or more )
abnormal QRS complexes . AV dissociation with occasional P waves
- SVT with bundle branch block may resemble VT on ECG
-Treatment is urgent:- i.v. class I amiodarone or
DC cardioversion (100 Joules)
45.
SVT versus VT
PSVTP wave to QRS complex bear 1:1 ratio, retrograde P wave
Fusion or capture beat in VT
In PSVT with aberrancy, the initial deflection of the QRS complex is
usually in the same direction as that of the normal QRS complex. In VT
the initial deflection is often in opposite direction.
Carotid massage works in PSVT , no effect in VT.
Cannon A waves in VT, not in PSVT.
46.
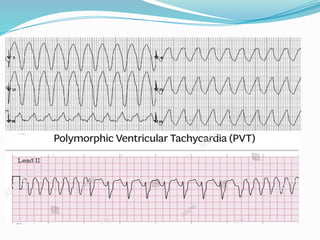
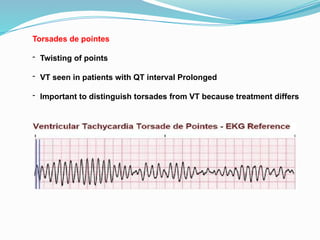
Torsades de pointes
-Twisting of points
- VT seen in patients with QT interval Prolonged
- Important to distinguish torsades from VT because treatment differs
48.
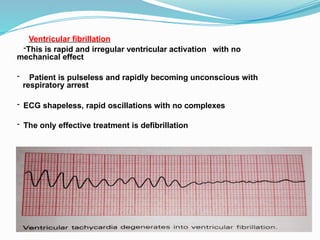
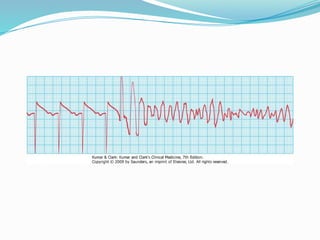
Ventricular fibrillation
-This israpid and irregular ventricular activation with no
mechanical effect
- Patient is pulseless and rapidly becoming unconscious with
respiratory arrest
- ECG shapeless, rapid oscillations with no complexes
- The only effective treatment is defibrillation
50.
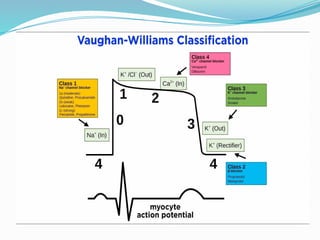
Antiarrhythmic drugs
Classification
Class I( sodium channel blockers )
Ia Disopyramide, Quindine
Ib Lidocaine, mexiletine
Ic Flecanide, propafenone
Class II ( Beta- blockers ) e.g.
Atenolol ,propranolol
Class III ( Prolong action potential ) e.g.
Amiodarone, sotalol
Class IV ( Calcium- channel blockers ) e.g.
Verapamil, Diltiazem
( Others Adenosine, Digoxin)






![Cardiccccac Arrhythmias [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cardiacarrhythmiasautosaved-241108153215-72acce97-thumbnail.jpg?width=640&height=640&fit=bounds)











































