Downloaded 74 times

















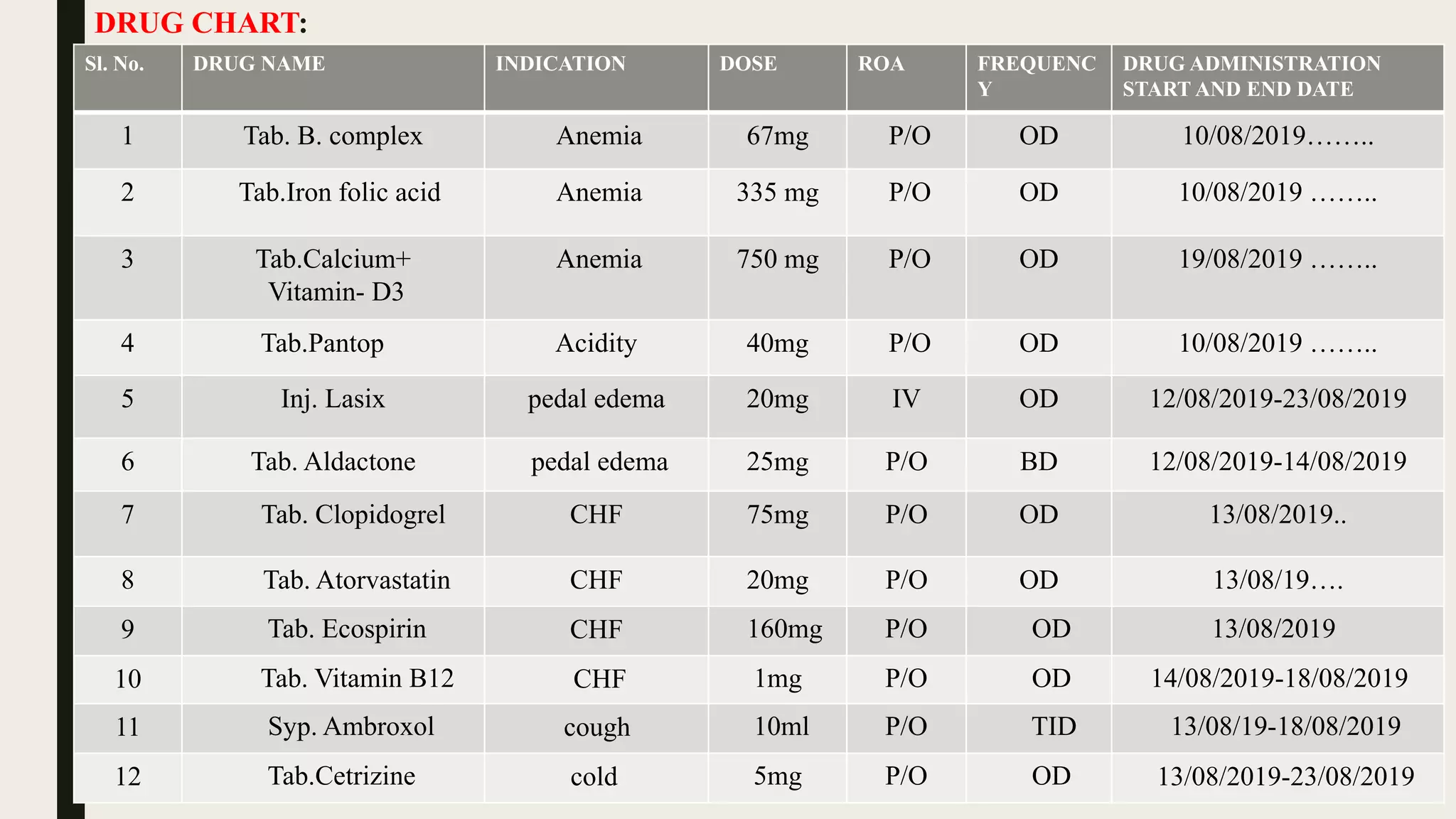


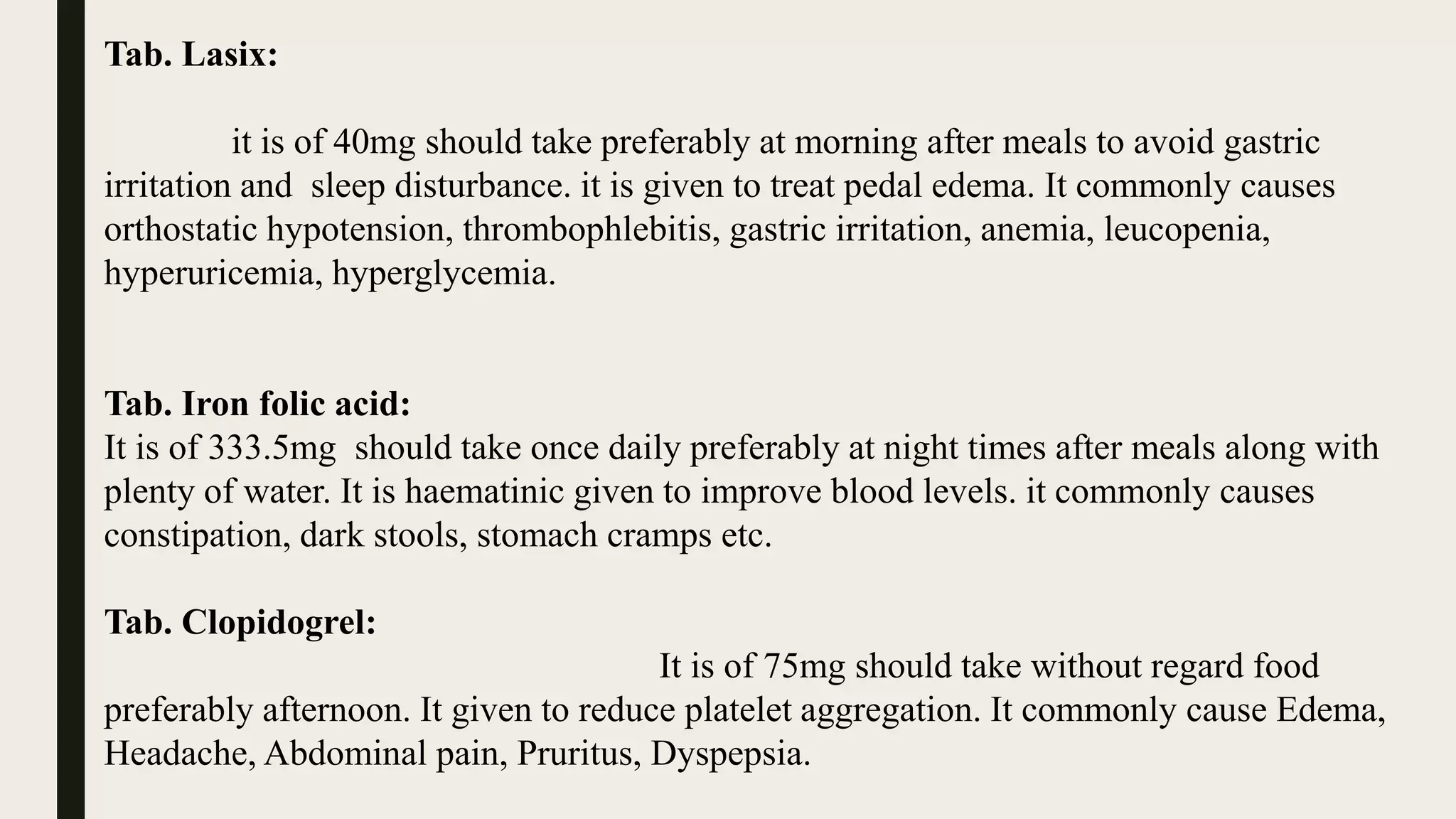






The document presents a case study of a 60-year-old female patient admitted with anemia and congestive heart failure. Over the course of her 14-day hospital stay, she was treated with medications to manage her symptoms, including lasix, iron supplements, B vitamins, and medications for heart failure. Her condition gradually improved and she was discharged on medications including lasix, iron, pantoprazole, and medications for congestive heart failure.























































































