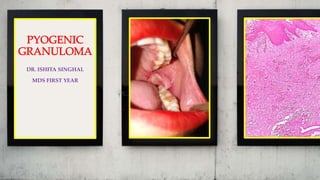
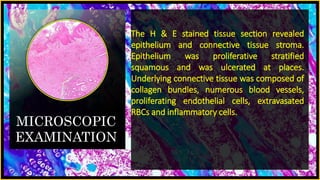
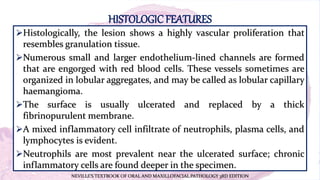
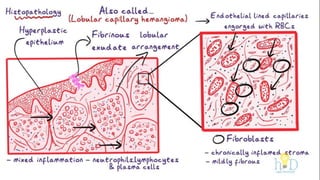
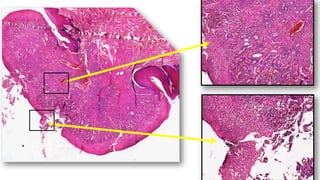
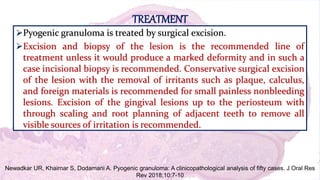
The document presents a medical case study of a 36-year-old female patient with a complaint of pain and swelling in the lower left back tooth area, diagnosed with pyogenic granuloma after an excisional biopsy. The histopathological examination showed a highly vascular proliferation resembling granulation tissue with inflammatory cells. Treatment recommendations include surgical excision of the granuloma and removal of irritants.







































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)








![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)








