
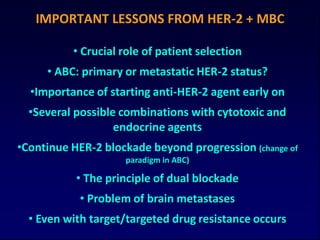
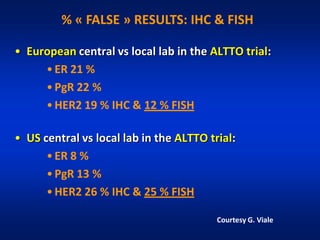
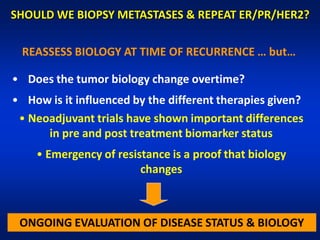
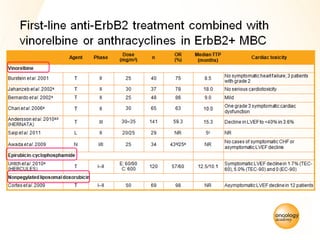
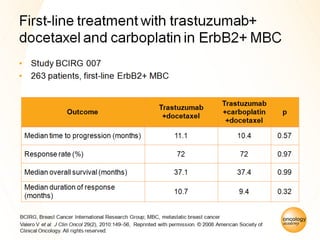
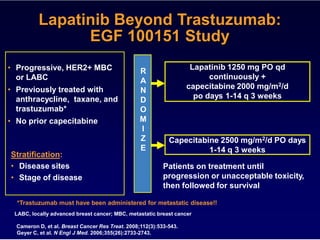
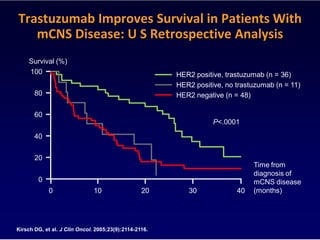
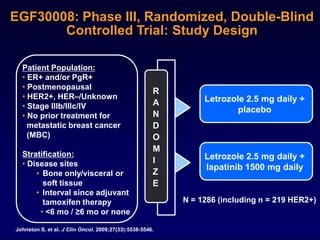
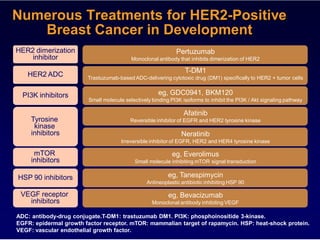
![TAnDEM Study: Randomized, Open-Label Trial of Anastrozole
± Trastuzumab in Advanced HER2+, HR+ Breast Cancer
Anastrozole
Anastrozole +
N = 207 Trastuzumab
Median age 55 years
Visceral disease 1/3
Prior chemo 1/2 Cross-over
70%
6.8% Response rate 20.3% P = .018
2.4 m Median PFS 4.8 m HR = 0.63; P = .0016
23.9 m Median OS 28.5 m P = .325
28.6 m Median OS 34.1 m
for patients with centrally P = .451
confirmed HR status
Trastuzumab added to anastrozole RR, PFS, TTP and CBR
Mackey JR, et al. Breast Cancer Res Treat. 2006;100(Suppl 1): Abstract 3.
Kaufman B, et al. J Clin Oncol. 2009 Sept 28. [Epub ahead of print].](https://image.slidesharecdn.com/cardosoher-2standard-of-care-111123061505-phpapp01/85/ABC1-F-Cardoso-HER-2-advanced-breast-cancer-State-of-the-art-management-of-HER-2-disease-12-320.jpg)
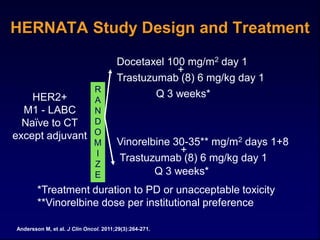
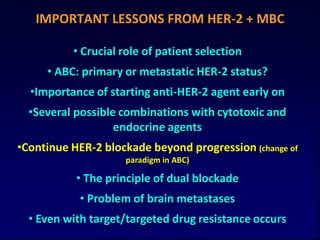
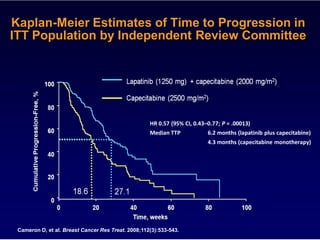
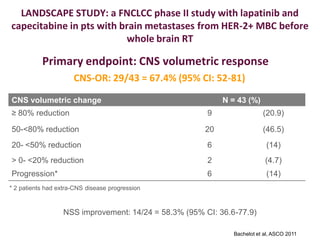
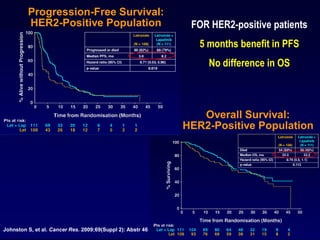
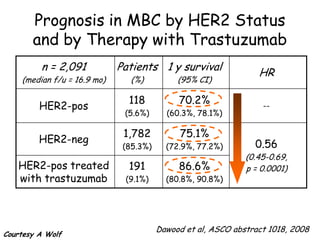
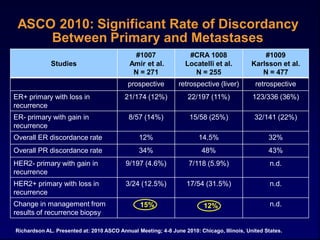
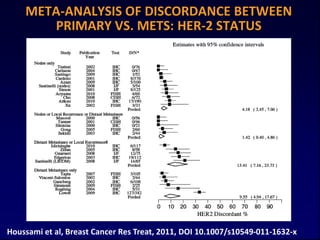
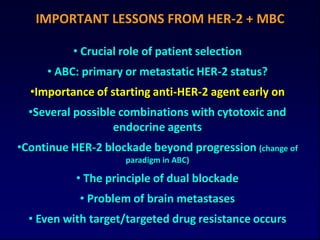
![Significant Rate of Discordancy
Between Primary and Metastases
Amir Curigliano
2010 Studies Karlsson Lindstrom
(n~270) (n~250)
Comparing Primary (n~470) (n~118-459)
Prospective Retrospective
to Metastasis Retrospective3 Retrospective4
Reanalyzed1 Liver Only2
ER+ ER- 12% 11% 36% 26%
ER- ER+ 14% 25% 22% 7%
HER2- HER2+ 5% 6% nd 7%
HER2+ HER2- 12% 32% nd 3%
1. Amir E, et al. J Clin Oncol. 2010;28(15S): Abstract 1007. 2. Curigliano G, et al. Ann Oncol. 2011 Feb 22 [Epub ahead
of print]. 3. Karlsson E, et al. J Clin Oncol. 2010;28(15S): Abstract 1009. 4. Lindstrom LS, et al. Cancer Res. 2010;70(24
Suppl): Abstract S3-5.](https://image.slidesharecdn.com/cardosoher-2standard-of-care-111123061505-phpapp01/85/ABC1-F-Cardoso-HER-2-advanced-breast-cancer-State-of-the-art-management-of-HER-2-disease-41-320.jpg)

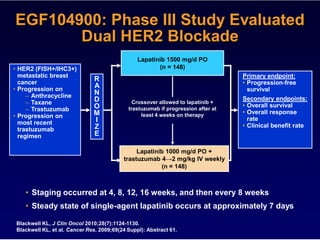
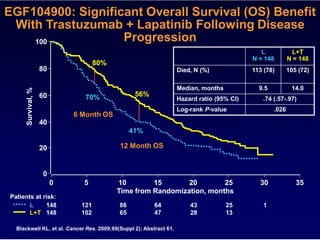
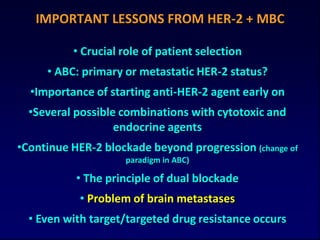
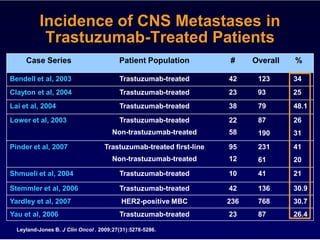
1) Reassessment of hormone receptor and HER2 status when breast cancer metastasizes can provide important information to guide treatment, as discordance rates between primary and metastatic tumors have been found to be as high as 30-50% for hormone receptors and 10-15% for HER2 in some studies. 2) Early administration of anti-HER2 targeted therapy for HER2-positive breast cancer is important, as several studies have shown improved outcomes when trastuzumab is started concurrently or shortly after diagnosis of metastatic disease rather than at later stages. 3) Continuing HER2-targeted therapy beyond progression on initial regimens provides clinical benefit, as evidenced by trials showing improved outcomes with extended trast






















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
