Treadmill test in cardiology
•
21 likes•7,224 views

Cardiac stress test is a cardiological test that measures the heart ability to respond to external stress in a controlled environment.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Treadmill test in cardiology
Similar to Treadmill test in cardiology (20)
Recently uploaded
Recently uploaded (20)
Treadmill test in cardiology
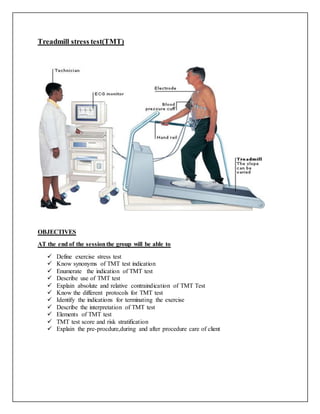
- 1. Treadmill stress test(TMT) OBJECTIVES AT the end of the sessionthe group will be able to Define exercise stress test Know synonyms of TMT test indication Enumerate the indication of TMT test Describe use of TMT test Explain absolute and relative contraindication of TMT Test Know the different protocols for TMT test Identify the indications for terminating the exercise Describe the interpretation of TMT test Elements of TMT test TMT test score and risk stratification Explain the pre-procdure,during and after procedure care of client
- 2. INTRODUCTION Exercise is a common physiological stress used to elicit cardiovascular abnormalities not present at rest and to determine adequacy of cardiac function. TMT is the one of the most frequent noninvasive modalities used to assess patients with suspected or proven cardiovascular disease. ETT has been quoted as having a sensitivity of 78% and a specificity of 70% in detecting coronary artery disease (CAD). In the clinical setting, the major indications for exercise testing are the diagnosis and prognostication of heart disease Alternative Names Exercise ECG; ECG - exercise treadmill; EKG - exercise treadmill; Stress ECG; Exercise electrocardiography; Stress test - exercise treadmill DEFINITION It is used to estimate the prognosis and to determine functional capacity, the likelihood and extent of CAD & effects of therapy. Treadmill test is also called a stress test, exercise electrocardiogram, graded exercise test, or stress ECG. It is used to provide information about how the heart responds to exertion. It usually involves walking on a treadmill at increasing levels of difficulty, while electrocardiogram, heart rate, and blood pressure are monitored. Uses of TMT Treadmill test is use to • Determine if there is adequate blood flow to heart during increasing levels of activity. • Evaluate the effectiveness of heart medications to control angina and ischemia. • Determine the likelihood of having coronary heart disease and the need for further evaluation. • Check the effectiveness of procedures done to improve blood flow within the heart vessels in people with coronary heart disease. • Identify abnormal heart rhythms. • Help to develop a safe exercise program CONTRAINDICATIONS • Acute myocardial infarction (within 2 days) • High-risk unstable angina • Symptomatic severe aortic stenosis • Symptomatic heart failure
- 3. • Acute pulmonary embolus or pulmonary infarction • Acute myocarditis or pericarditis • Acute aortic dissection • Electrolyte abnormalities • Tachy or Brady arrhythmias • Mental or physical impairment • Hypertension (>200/100 at rest) • Neuromuscular and musculoskeletal disorder exacerbated by exercise INDICATIONS 1. Diagnosis of coronary artery disease (CAD) in patients with chest pain that is atypical for myocardial ischemia 2. Assessment of functional capacity and prognosis of patients with known CAD 3. Assessment of prognosis and functional capacity of patients with CAD soon after uncomplicated myocardial infarction (before hospital discharge or early after discharge) 4. Evaluation of patients with symptoms consistent with recurrent, exercise-induced cardiac arrhythmias 5. Assessment of functional capacity of selected patients with congenital or valvular heart disease 6. Evaluation of patients with rate-responsive pacemakers 7. Evaluation of asymptomatic men >40 years with special occupations (airline pilots, bus drivers, etc) 8. Evaluation of asymptomatic individuals >40 years with two or more risk factors for CAD 9. Evaluation of sedentary individuals (men >45 years and women >55 years) with two or more risk factors who plan to enter a vigorous exercise program 10. Assessment of functional capacity and response to therapy in patients with ischaemic heart disease or heart failure 11. Monitoring progress and safety in conjunction with rehabilitation after a cardiac event or surgical procedure RISKS AND CONTRAINDICATIONS • Risks of MI and death 1/2500. Absolute Contraindications (ACC/AHA guidelines) Acute MI (48 hrs) – Unstable angina not stabilized by medical therapy Cardiac arrhythmia causing syx or hemodynamic compromise. Symptomatic severe AS. Uncontrolled CHF Acute pulmonary embolus. – Acute myocarditis or pericarditis. Acute aortic dissection
- 4. Relative Contraindications LM CAD Moderate stenotic valvular disease Electrolyte abnormalities SBP>220, DBP>110. Tachy or brady arrhythmia HOCM or other forms of LVOT obstructions Mental instability High degree AV Block TREADMILL PROTOCOL Exercise capacity is reported in terms of estimated metabolic equivalents of task (METs). The MET unit reflects the resting volume oxygen consumption per minute (VO2) for a 70-kg, 40-year-old man, with 1 MET equivalent to 3.5 mL/min/kg of body weight. METs = Speed x [0.1 + (Grade x 1.8)] + 3.5 3.5 In the standard Bruce protocol, the starting point (ie, stage 1) is 1.7 mph at a 10% grade (5 METs). Stage 2 is 2.5 mph at a 12% grade (7 METs). Stage 3 is 3.4 mph at a 14% grade (9 METs). This protocol includes 3-minute periods to allow achievement of a steady state before workload is increased. The modified Bruce protocol has 2 warmup stages, each lasting 3 minutes. The first is at 1.7 mph and a 0% grade, and the second is at 1.7 mph and a 5% grade. This protocol it is most often used in older individuals or those whose exercise capacity is limited by cardiac disease. The Bruce protocol has larger increments between stages than do other protocols, such as the Naughton, Weber, and Asymptomatic Cardiac Ischemia Pilot (ACIP) study protocols, all of which start with less than 2 METs at 2 mph and increase in 1- to 1.5-MET increments between stages.Bruce protocol include • Total of 1+6 (Seven 3 minute stages) – (3+18 min) • Each minute exercise is approximately 1 MET • Pretest plain walking + 6 Stages of graded exercise • In each stage there is increase in speed and gradient • Initial 1.7 mph with 10% gradient (upward inclination) • Maximum 5.5 mph with 20% gradient
- 5. Other exercise protocols include bicycle and arm ergometry, both of which are used less often in North America than treadmill stress testing is. The bicycle ergometer has the advantage of requiring less space than a treadmill. It is quieter, permits sensitive precordial measurements without much motion artifact, and is generally safer because the risk of falling from the machine is lower. Stage Minutes % grade km/h MPH METS 1 3 10 2.7 1.7 5 2 6 12 4.0 2.5 7 3 9 14 5.4 3.4 10 4 12 16 6.7 4.2 13 5 15 18 8.0 5.0 15 6 18 20 8.8 5.5 18 7 21 22 9.6 6.0 20 As the Bruce Protocol Treadmill test is a maximal fitness test, you have to run continuously until you are tired. The result is the maximum time in minutes spent on the test. VO2 max is calculated using a formula and the recorded minutes. Due to this, the test is also known as an indirect test. The total time (T) on the treadmill is measured as a part of a minute. For instance, 9 minutes and 30 seconds will be noted as T=9.5. Results of this test are measured using different formulas for women and men. • Women VO2max = 4.38 x T - 3.9 • Men VO2max = 14.8 - (1.379 x T) + (0.451 x T2) - (0.012 x T3) Modifications to the Test The Bruce Protocol Treadmill Test has been slightly modified for sedentary and elderly patients. This modified test begins at a lower workload compared to the standard test. Here, the first level is performed at 0% incline and 2.74 km/h. The second level is done at 5% incline and 2.74 km/h. The third level matches the first level of the Standard Bruce Protocol Test.
- 6. INDICATIONS FOR TERMINATION OF EXERCISE TESTING The American College of Cardiology (ACC)/American Heart Association (AHA) guidelines also specifies indications for termination of exercise testing. Absolute indications for termination of testing include the following: Drop in systolic blood pressure (SBP) of more than 10 mm Hg from baseline, despite an increase in workload, when accompanied by other evidence of ischemia Moderate-to-severe angina Increasing nervous system symptoms (eg, ataxia, dizziness, near-syncope) Signs of poor perfusion (cyanosis or pallor) Technical difficulties in monitoring electrocardiographic (ECG) tracings or SBP Subject’s desire to stop Sustained ventricular tachycardia ST elevation (> 1 mm) in leads without diagnostic Q waves (other than V 1 or aVR) RELATIVE INDICATIONS FOR TERMINATION INCLUDE THE FOLLOWING: Drop in SBP of 10 mm Hg or more from baseline, despite an increase in workload, in the absence of other evidence of ischemia ST or QRS changes such as excessive ST depression (horizontal or downsloping ST- segment depression >2 mm) or marked axis shift Arrhythmias other than sustained ventricular tachycardia, including multifocal premature ventricular contractions (PVCs), triplets of PVCs, supraventricular tachycardia, heart block, or brad arrhythmias Fatigue, shortness of breath, wheezing, leg cramps, or claudicating
- 7. Development of bundle branch block or intraventricular conduction delay that cannot be distinguished from ventricular tachycardia Increasing chest pain Hypertensive response (SBP of 250 mm Hg, diastolic blood pressure [DBP] higher than 115 mm Hg, or both) INTERPRETATION OF TEST FINDINGS Interpretation should include exercise capacity and clinical, hemodynamic, and ECG response. The occurrence of ischemic chest pain consistent with angina is important, particularly if it forces termination of the test. The classic criteria for visual interpretation of positive stress test findings include the following: : Clinical, hemodynamic, and ECG response. The patient is normally considered to have been adequately 'stressed' if they achieve 85% or more of their maximum heart rate J point – This is defined as the junction of the point of onset of the ST-T wave; it is normally at or near the isoelectric baseline of the ECG ST80 – This is defined as the point that is 80 msec from the J point Depression of 0.1 mV (1 mm) or more ST-segment slope within the range of ± 1 mV/sec in 3 consecutive beats Non-coronary causes of ST depression. Severe hypertension Severe aortic stenosis Cardiomyopathy Anemia Hypokalemia Severe hypoxia Digitalis Sudden excessive exercise Glucose load Left ventricular hypertrophy Intraventricular conduction delay Elements Of Interpretation • ECG Types of ST Segement Displacement Measurement of ST Segement is very important In myocardial ischemia, ST segment becomes horizontal, with progressive exercise depth of ST segment may increase In immediate post recovery phase ST segment displacement may persist with down sloping ST segments and T wave inversion returning to baseline after 5- 10 min .In 10% , ischemic response may appear in recovery phase Hyperventilation Mitral valve prolapse Intraventricular conduction delay Preexcitation syndrome ( Wolff- Parkinson-White [WPW] syndrome) Severe volume overload (aortic, mitral regurgitation) Supraventricular tachyarrhythmias
- 8. Measurements of ST Segment Displacement PQ junction is chosen as isoelectric point , TP segment is true isoelectric point but impractical choice Development of 0.1mv (1mm) or greater of ST segment depression measured from PQ junction with a relatively flat ST segment slope (e.g. <0.7-1mv /sec), 80 msec after J point (ST 80) in 3 consecutive beats with a stable base line is considered to be abnormal response .When ST 80 measurement is difficult to determine at rapid heart rates ST 60 measurements should be used when ST segment is depressed at rest, j point or ST 80 measurements should be depressed an additional 0.1mv or more, to consider abnormal Upsloping ST segment In patients with high CAD prevalence, slow up sloping ST segment depressed 0.15mv or greater at 80msec, after J point is considered abnormal ST segment elevation Development of 0.1mv ( 1mm) or greater of J point elevation, at 60msec after J point in 3 consecutive beats with stable baseline is considered abnormal response. Occurs in 30% of AWMI & 15% of IWMI When it occurs in non q wave lead in a patient without previous MI it indicates transmural ischemia caused by coronary spasm or high grade coronary narrowing. ST elevation is relatively specific for territory of ischemia
- 10. • BLOOD PRESSURE Normal exercise response is to increase systolic BP Progressively with increasing workloads. In normal persons diastolic BP doesn’t change significantly Failure to increase systolic BP beyond 120mm Hg, or a sustained decrease greater than 10 mmHg is abnormal • HEART RATE Sinus rate increases progressively with exercise.
- 11. Inappropriate increase in heart rate at low exercise work loads may occur in patients who are in AF,physically deconditioned, hypovolumic, anemic, or have marginal left ventricular function Chest discomfort Chest discomfort usually occurs after the onset of ST segment abnormality TREAD MILL (TM) SCORE: Is designed to provide survival estimates based on results from exercise test. Provides accurate prognostic & diagnostic information The Duke Treadmill Score is used for risk stratification with treadmill testing. Duke Treadmill Score (DTS): Risk Stratification RISK STRATIFICATION DTS Risk < –10 High (79% 4-year survival) –10 to +4 Moderate (95% 4-year survival) ≥ +5 Low (99% 4-year survival) #Exercise time should be In minutes on the Bruce protocol. ##Angina Index 0-if no angina 1-if typical angina occurs during exercise 2-if angina was the reason pt stopped exercise <5-low risk:no coronary art stenosis or svd-5yr survival of 97% -10 to+4 :-moderate risk --- 5yr survival of 91% >11– high risk: 3vd or Lt main CAD:- 5yr survival of 72% PREPROCEDURE CARE General concerns prior to performing an exercise test include 1. Patients should be instructed not to drink,eat caffeinated beverages or smoke 3hr before testing & to wear comfortable shoes and clothes. 2. Unusual physical exertion should be avoided TM score: Exercise time-(5*ST deviation)-(4*treadmillangina index)
- 12. 3. Brief history & physical examination should be performed 4. Should be instructed about risks and benefits 5. Informed consent is taken 6. Area of electrode application should be rubbed with alcohol saturated pad to remove oil and rubbed with sand paper to reduce skin resistance to 5000ohms or less 7. Cables should be light flexible and shielded 8. Room temp should be 18 –24 C & humidity less than 60% 9. Safety precautions and equipments needs. Everything necessary for cardiopulmonary resuscitation must be available and regular drills should be performed to ascertain that both personnel and equipments are ready for a cardiac emergency. The treadmill should have front and side rails for subjects to steady themselves. A resuscitator cart, defibrillator and appropriate cardio active drugs should be available in the TMT room. 10. IV line should be started in high risk patients. DURING TMT TESTING Exercise test should be performed under the supervision of a physician who has been trained to conduct exercise tests. Following observation must be done during TMT 12 lead ECG is recorded with electrodes at the distal extremities Torso ECG is obtained in standing and sitting position Walking should be demonstrated to the patient HR, BP & ECG should be recorded at the end of each stage. Assessing appearance during the test If false +ve test is suspected, hyperventilation should be performed Subjects should be reminded not to grasp the front or side rails because this decreases the work performed and create noise in the ECG. Hanging on increases exercise time resulting in an over estimation of exercise capacity. At each stage each lead should be examined for: Planar ST depression (this can be difficult to delineate from depression of the J point, which is the point where the QRS complex meets the ST wave). 'Flipping' of the T waves. Arrhythmias. Examination of all leads should continue into the recovery stage after the exercise stage of the test has been completed.
- 13. Suboptimal Exercise (Setting Target Heart Rate) Exercise is the preferred method of stress for myocardial perfusion imaging, but some patients may not be able to exercise adequately for a variety of reasons. For exercise to be adequate for imaging, the patient must reach at least 85% of his or her maximal predicted heart rate,5 as estimated by the following equation1: 220 − Patient Age = Maximal Predicted Heart Rate Patient Effort Level: Perceived Exertion Below are 2 self-rating scales that can be used with patients to determine their levels of effort/exertion while exercising on the treadmill. Borg Rating of Perceived Exertion Scale (RPE) Heart rate can be approximated by multiplying the Borg RPE by a factor of 10.14 Actual heart rate can vary dependingonage and physical condition. AFTER TMT After TMT post test monitoring of the patient must be done and documentation is done. (Why test is terminated or findings of TMT Test).
- 14. COMPLICATIONS These are rare but can be fatal - eg, myocardial infarction, left ventricular rupture, ventricular fibrillation or ventricular tachycardia. CONCLUSION The exercise test continues to have an integral place in cardiovascular medicine because of its high yield of diagnostic, prognostic and functional information. In the clinical setting, the major indications for exercise testing are the diagnosis and prognostication of heart disease. The determination of exercise capacity is helpful in quantifying disability, estimating prognosis and monitoring the disease state of patients with chronic heart disease and known coronary heart disease. REFERNECES 1. Liibby P, Bonow RO, Mann DL, Zipes DP. Exercise stress testing. Braunwald E, ed. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 8th ed. Philadelphia, Pa: WB Saunders; 2007. 2. Botvinick EH. Current methods of pharmacologic stress testing and the potential advantages of new agents. J Nucl Med Technol. 2009 Mar. 37(1):14-25. [Medline]. 3. Cerqueira MD, Nguyen P, Staehr P, Underwood SR, Iskandrian AE. Effects of age, gender, obesity, and diabetes on the efficacy and safety of the selective A2A agonist regadenoson versus adenosine in myocardial perfusion imaging integrated ADVANCE- MPI trial results. JACC Cardiovasc Imaging. 2008 May. 1(3):307-16. [Medline]. 4. Feil H, Seigel ML. Electrocardiographic changes during attacks of angina pectoris. Am J Med Sci. 1928. 175:255