
Downloaded 47 times







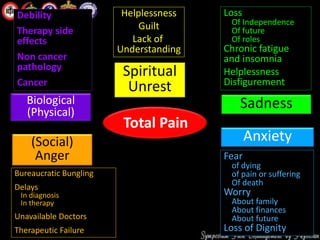
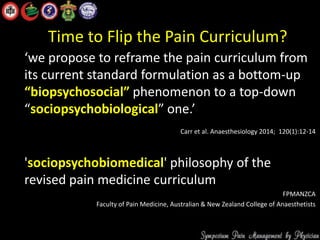
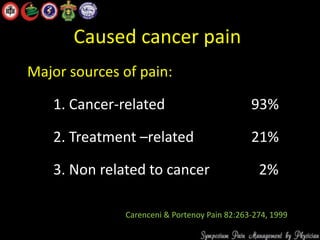
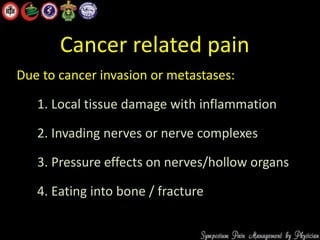
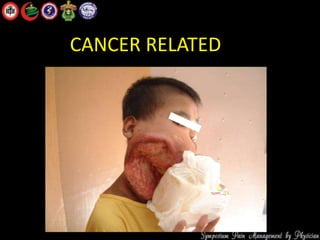

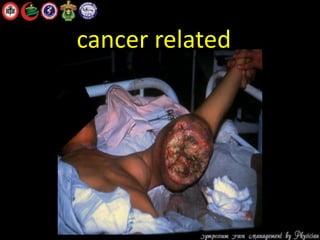









The document discusses the complex nature of cancer pain, emphasizing its invisibility and subjective experience, which can lead to severe emotional distress and considerations of suicide among patients. It outlines the various sources of cancer pain, including biological, psychological, social, and spiritual factors, and highlights the importance of thorough assessment and management strategies. The text also advocates for a revised educational approach to pain management that emphasizes a sociopsychobiological perspective.























































































