Downloaded 32 times


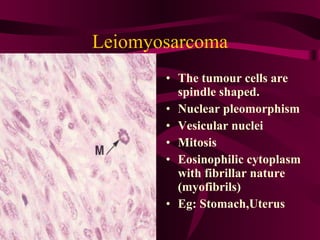

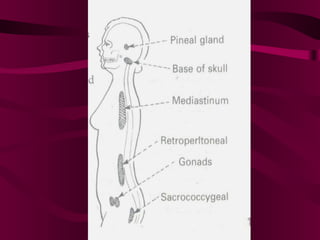



There are several types of malignant connective tissue tumors (sarcomas) that can develop at any age, though they are less common than carcinomas. Sarcomas spread through the bloodstream and are made up of neoplastic cells merged into the surrounding tissue (stroma). Examples include fibrosarcomas, osteosarcomas, rhabdomyosarcomas, and leiomyosarcomas. Teratomas are tumors composed of multiple tissue types from different germ layers arranged chaotically. They most commonly occur in the ovaries and testes of young and middle-aged individuals. While usually benign, teratomas can rarely become malignant.