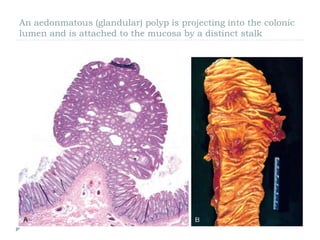
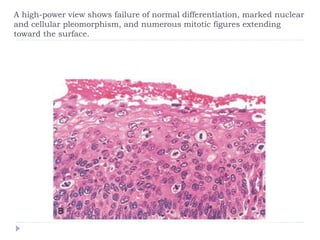
This document provides information on neoplasia and the classification of tumors. It defines neoplasia as new abnormal growth and discusses the distinction between benign and malignant tumors. Benign tumors are self-limited, do not invade or spread, and can be surgically removed. Malignant tumors invade nearby tissue and metastasize to distant sites. The document outlines different types of benign and malignant tumors based on cell of origin and characteristics. It also discusses features of tumor differentiation, anaplasia, and cellular changes seen in malignant tumors.