
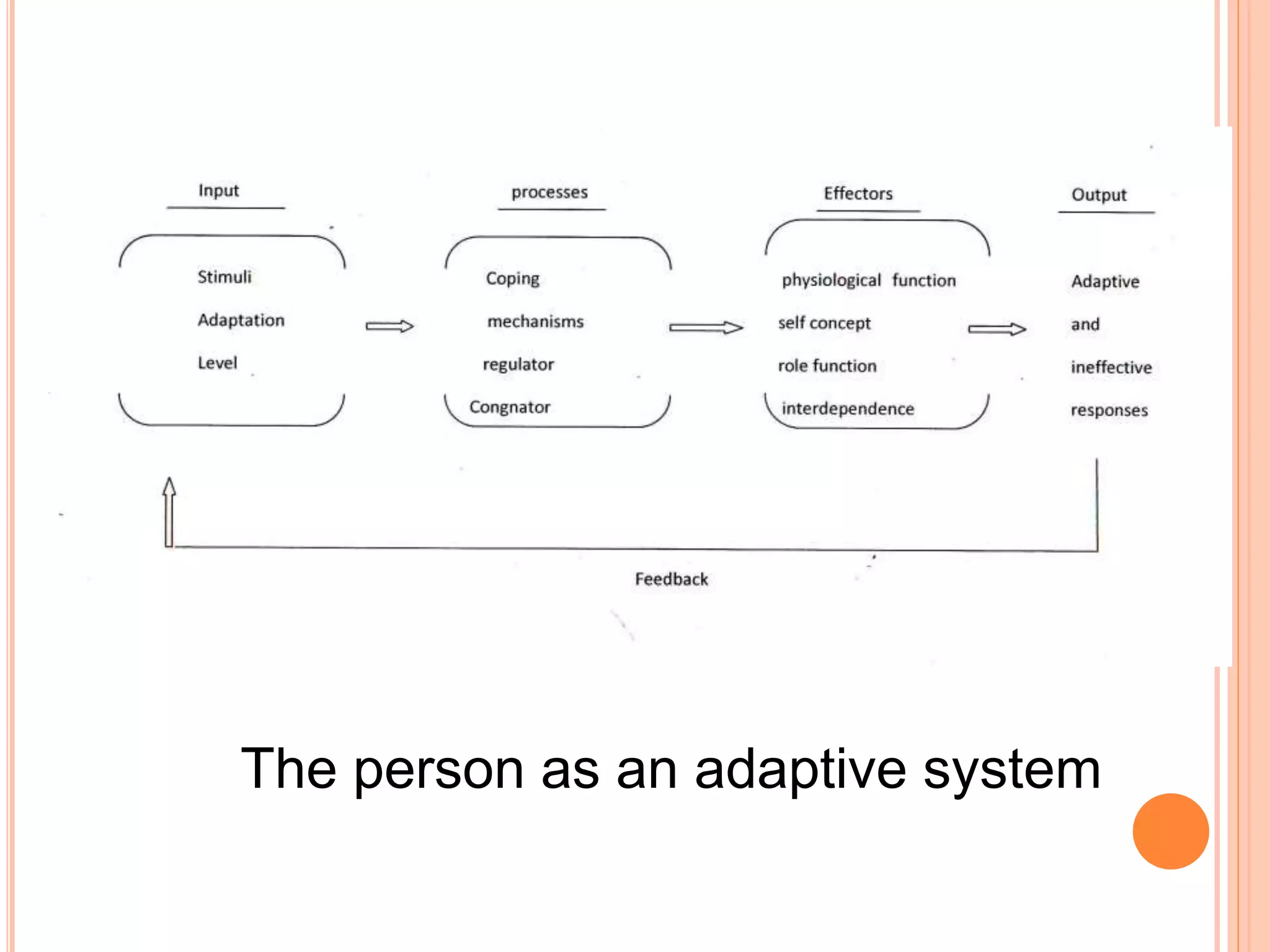

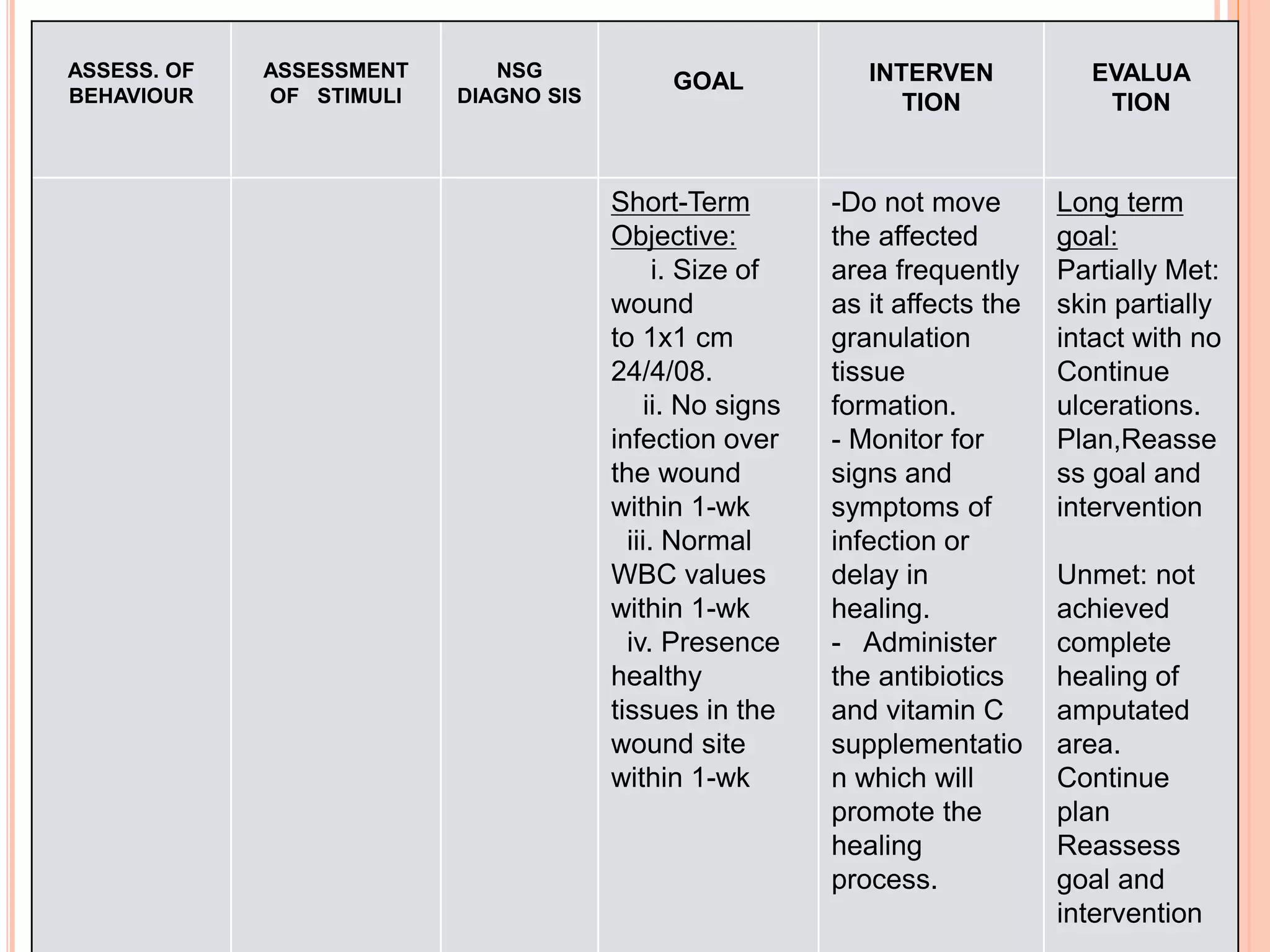
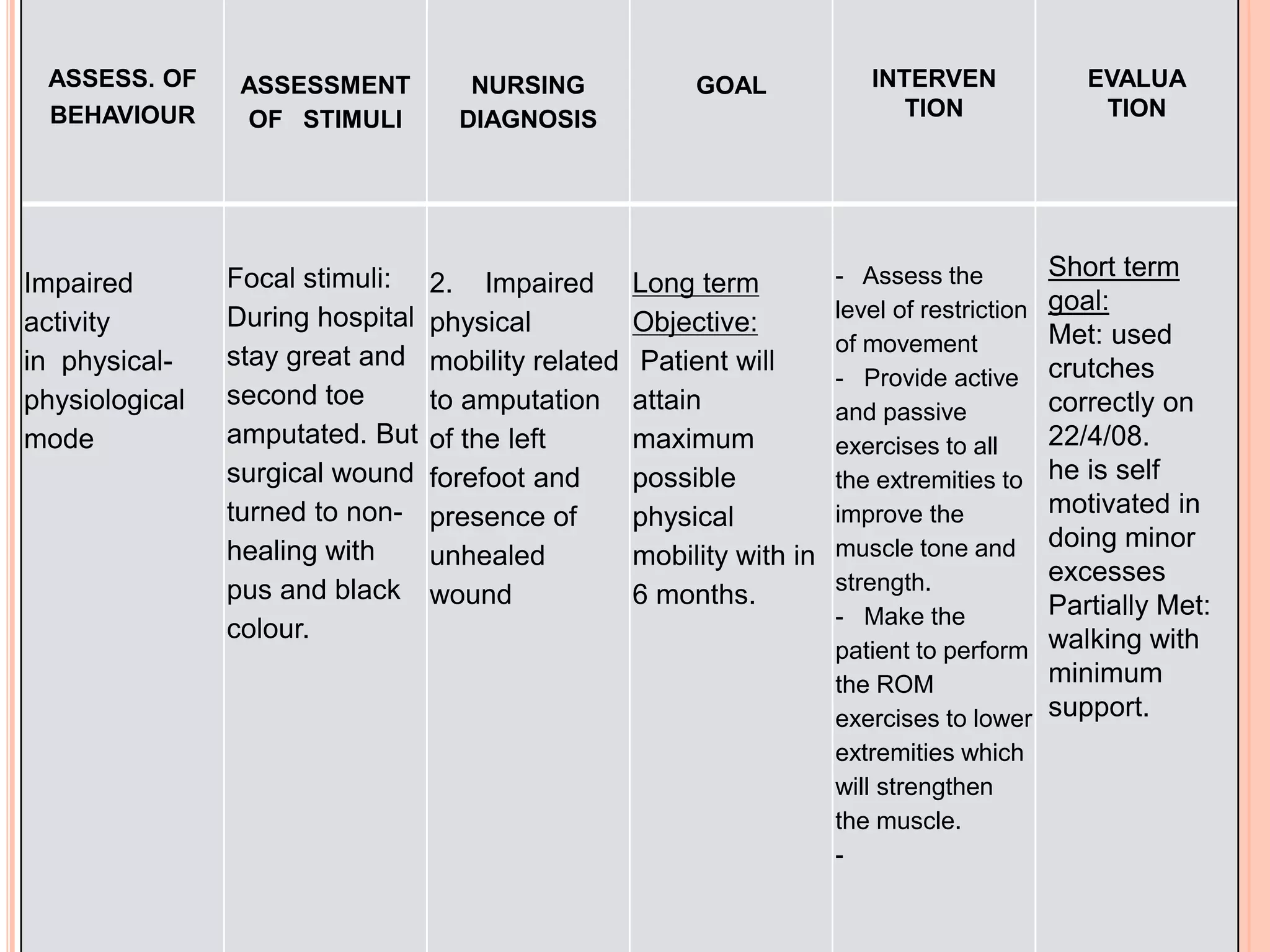
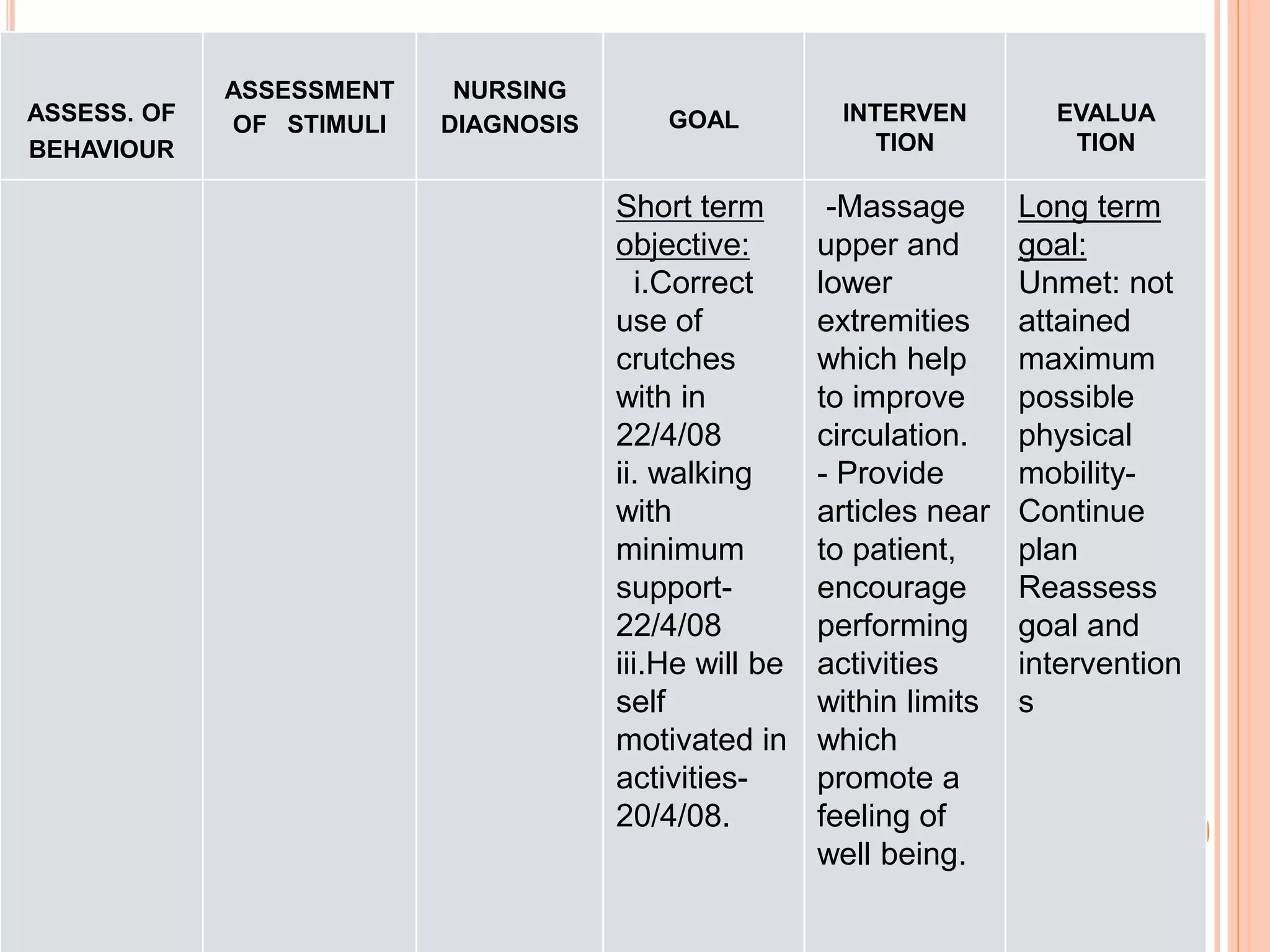


Sister Callista Roy's adaptation model emphasizes nursing as a scientific discipline focused on helping individuals adapt to health and illness through four adaptive modes: physiological needs, self-concept, role function, and interdependence. The model incorporates the interaction between individuals and their environment, requiring nurses to assess stimuli affecting a person's adaptation and facilitate adaptive responses. Roy's framework serves as the basis for nursing education, practice, and research, highlighting the importance of understanding patients as holistic adaptive systems.